

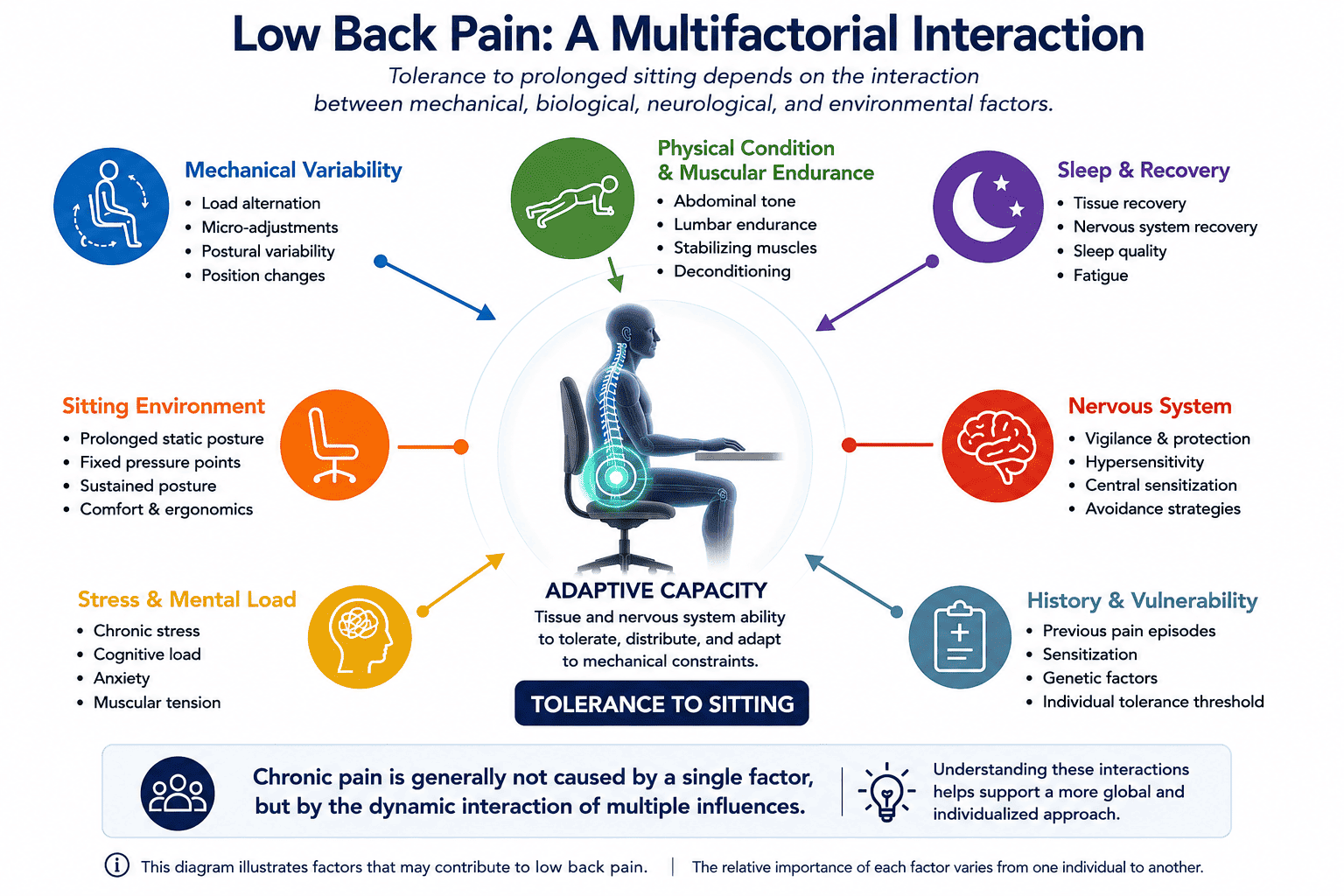
Back pain rarely has a single cause. In most cases, it results from a complex interaction between mechanical stress, prolonged sitting, sleep quality, physical activity, stress levels, and nervous system sensitivity. In addition, the intrinsic ability of tissues to tolerate repeated loading plays a central role.
Within this multifactorial framework, tissue adaptability remains largely underestimated. When the body stays seated for prolonged periods in a rigid configuration, tissues may progressively lose part of their adaptive capacity. Muscles, fascia, and sensory receptors then struggle to distribute loads efficiently. The goal is therefore not to identify a single culprit, but rather to restore an environment that supports movement, adaptability, and postural self-regulation.
The human body possesses a remarkable ability to adapt. Muscles, bones, fascia, and the nervous system constantly remodel themselves according to the mechanical stresses they experience.
This adaptive plasticity is one of the body’s greatest strengths. It allows tissues to adjust, compensate, and reinforce themselves in order to preserve functional balance throughout daily life.
However, this same plasticity can become detrimental when the environment imposes monotonous and prolonged constraints. Prolonged sitting, for example, reduces pelvic mobility and limits natural micro-adjustments. Over time, this loss of movement variability may progressively diminish the adaptive strategies of the locomotor system.
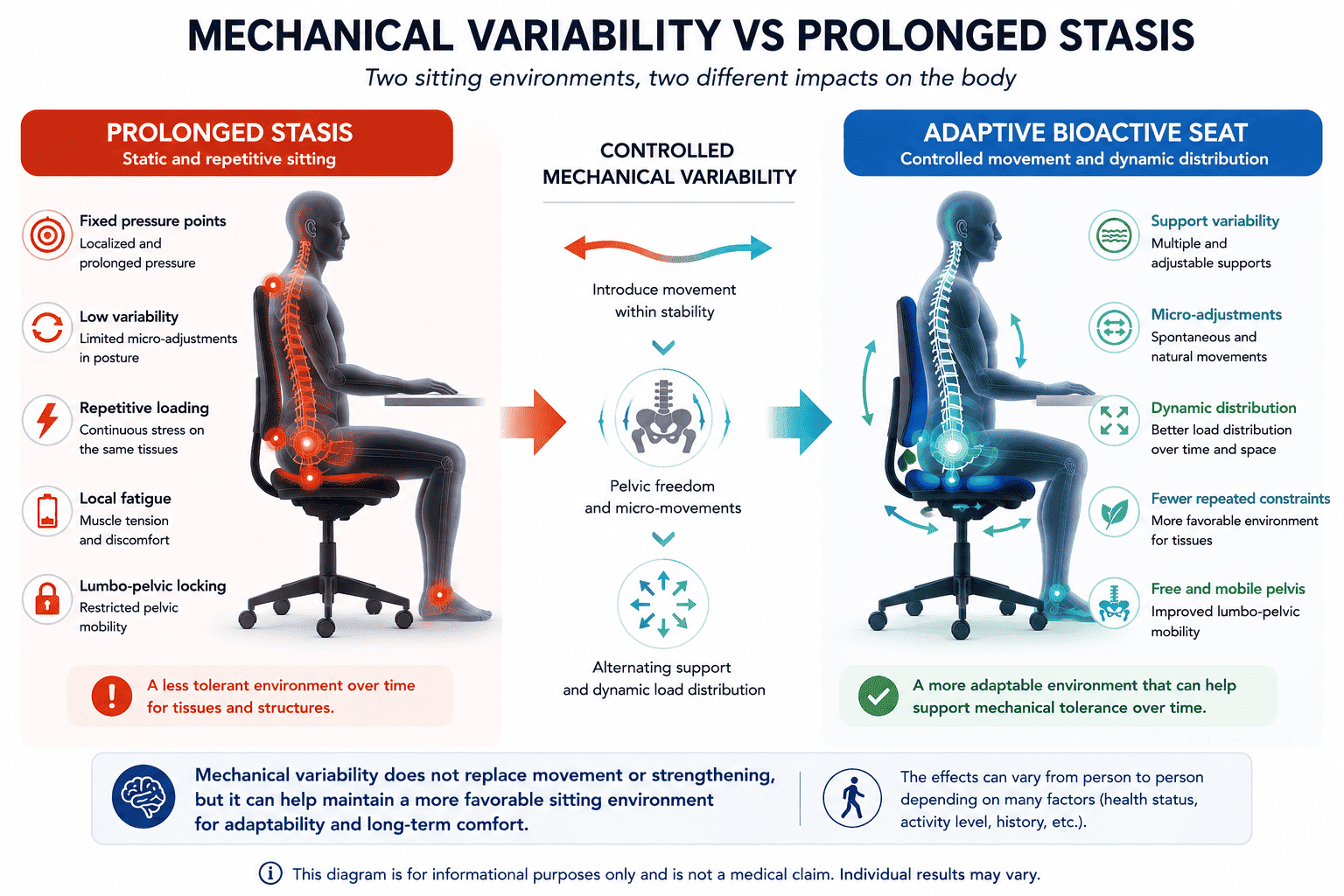
In practice, the problem is not simply “sitting badly.” The real issue lies in remaining too long in a fixed configuration. The same tissues remain under continuous stress, with fewer opportunities to alternate between compression, release, gliding, and recovery.
Important: This article provides a biomechanical and tissue-based perspective on back pain related to prolonged sitting. It does not replace medical advice. Persistent, progressive, or night pain should always be evaluated by a healthcare professional, especially when associated with weakness, fever, or neurological symptoms.
1. Back Pain Is a Multifactorial Condition
Modern research increasingly recognizes back pain as a complex and multifactorial condition. Several biological, mechanical, neurological, and behavioral dimensions interact simultaneously. Structural findings visible on imaging are often insufficient to fully explain either pain intensity or functional limitations.
Some individuals show significant disc degeneration on MRI with very little pain, while others experience disabling symptoms despite reassuring imaging results. This discrepancy clearly demonstrates that pain cannot be explained solely by visible structural abnormalities.
1.1 Biological, Mechanical, and Nervous System Factors
On a biological level, several mechanisms interact continuously. Local irritation, mechanical overload, reduced mobility, low-grade inflammation, muscular deconditioning, and nervous system hypersensitivity frequently influence one another.
Fascia and connective tissues also play a major role. When deprived of movement, fascia progressively loses part of its gliding capacity. Tissues become less mobile, less hydrated, and less tolerant to prolonged mechanical stress.
1.2 Behavioral and Psychosocial Factors
Sleep quality, chronic stress, inactivity, fear of movement, and professional tension can also contribute to persistent pain. These dimensions interact with the nervous system and may reinforce protective muscular strategies and pain sensitivity.
In other words, tissue adaptability is not the sole explanation for back pain. Rather, it represents one important component within a broader adaptive system involving the body, the nervous system, lifestyle habits, and the sitting environment.
2. Loss of Adaptability: A Possible Contributor to Chronic Pain
Chronic sitting-related pain does not always appear suddenly. In many cases, it develops progressively through the accumulation of repeated low-level mechanical stress.
Within this context, loss of adaptability refers to a reduced ability of tissues to tolerate load variations, glide over one another, and recover efficiently after mechanical stress.
2.1 Davis’s Law and Soft Tissue Remodeling
According to Davis’s Law, soft tissues remodel themselves according to the mechanical forces regularly imposed upon them. Tissues exposed to varied movements tend to preserve greater flexibility and adaptability.
Conversely, prolonged static loading tends to promote a more rigid organization. Over time, tissues become less mobile and less tolerant to changes in posture.
During prolonged sitting, posterior muscular chains, lumbar fascia, and gluteal tissues remain under continuous loading. This mechanical monotony progressively reduces tissue variability and adaptive reserve.
2.2 Sensory Deprivation and Reduced Variability
Tissues are not merely mechanical structures — they are also sensory organs. Fascia, muscles, and ligaments contain numerous mechanoreceptors that continuously inform the nervous system about pressure, stretch, and movement.
When the sitting environment generates little variability, these receptors provide repetitive and monotonous sensory input. As a result, the nervous system may progressively lose perceptual precision in certain regions, particularly around the pelvis and lower back.
This sensory impoverishment does not directly create pain, but it may contribute to a less adaptable and more reactive mechanical environment.
2.3 Vulnerability Factors and Recovery Capacity
A reduction in tissue variability does not automatically lead to chronic pain. Some individuals maintain good tolerance despite substantial constraints, while others become symptomatic much more rapidly.
This vulnerability depends on a complex interaction between body mechanics, sleep quality, physical activity, stress levels, inflammatory status, and nervous system sensitivity.
Loss of tissue adaptability should therefore not be viewed as a single universal cause of back pain, but rather as one potential contributor capable of reducing the body’s margin of tolerance.
3. Why Mechanical Variability Matters
The human body rarely tolerates complete immobility well. Even at rest, it continuously performs subtle unconscious oscillations and small pressure shifts. This natural variability is essential for tissue health.
3.1 Compression, Release, and Fluid Exchange
Intervertebral discs and fascia depend directly on pressure variations. These regular mechanical changes facilitate fluid exchange, hydration, and proper tissue behavior.
Alternating compression and release acts like a biological pump. It supports fluid circulation, reduces local congestion, and helps maintain tissue flexibility.
Conversely, prolonged static loading may generate sensations of stiffness, crushing, numbness, or deep discomfort, particularly in individuals already sensitive to prolonged sitting.
3.2 Preventing Local Fatigue
Remaining in the same position continuously loads the same muscles and support zones. This lack of alternation increases local fatigue and protective muscular tension, progressively reducing sitting tolerance.
Changing support points regularly helps redistribute mechanical stress across different tissues and muscular groups, limiting overload on a single region.
Postural variability therefore does not mean constant movement. Rather, it refers to a continuous sequence of subtle micro-adjustments that help the body remain active, adaptable, and responsive.
4. Tissue Adaptability Within the SBNFA™ Doctrine
The SBNFA™ doctrine (Systemic Biological Neuro-fascial Adaptive) proposes a global understanding of prolonged sitting. Within this framework, structural mechanics, fascia, nervous system regulation, and adaptive capacity are studied together.
This approach does not attempt to explain all pain through a single mechanism. Instead, it highlights a frequently overlooked factor: the quality of the mechanical environment in which the body spends several hours each day.
4.1 Restoring a More Favorable Mechanical Environment
Adaptability does not mean instability. In order to move without excessive protective tension, the body first requires stable and secure support.
Seat height, knee positioning, pelvic orientation, and respect for the individual’s natural spinal profile all influence mechanical stress distribution around the lumbar-pelvic complex.
The objective is therefore not to impose one “perfect posture,” but rather to reduce unnecessary constraints and restore freedom of movement to the pelvis and spine.
4.2 Reintroducing Variability Without Losing Stability
Once a stable framework has been established, the next challenge is to reintroduce controlled movement variability. This is precisely the principle behind bioactive seating systems such as Aporia®, developed around four independent articulated pads.
These independent support zones accompany subtle pelvic and thigh movements. The goal is not to create instability, but rather to maintain gentle and continuous mechanical variability.
Mechanically, this variability may help redistribute pressure, reduce prolonged fixed points, stimulate sensory receptors, and maintain fascia gliding.
Of course, no seating system can guarantee immediate pain relief. Rather, this type of approach seeks to create conditions that may support the body’s natural self-regulation mechanisms.
5. What This Approach Does Not Replace
Improving the sitting environment represents an important biomechanical lever, but it cannot replace the other essential pillars of spinal health.
International medical guidelines consistently emphasize the importance of maintaining daily movement, preserving mobility, adapting physical activity, and addressing psychosocial factors.
A well-designed ergonomic or bioactive seat should therefore always be integrated into a broader health strategy that includes:
- daily movement and walking,
- regular standing breaks,
- progressive strengthening exercises,
- adequate restorative sleep,
- stress management,
- medical or physiotherapy follow-up when necessary.
In summary, tissue adaptability should not be presented as the single explanation for back pain. Rather, it represents a highly relevant biomechanical perspective within a comprehensive, multifactorial, and individualized model of chronic pain.
Further Reading
-
Why Can You Experience Pain Despite a Normal MRI?
Discover why chronic pain may persist despite reassuring imaging findings and how invisible functional mechanisms may contribute to ongoing symptoms. -
Why Moving a Little Matters More Than Moving a Lot
Explore how micro-movements support tissue drainage, movement variability, and pain regulation while sitting. -
Understanding Fascia and Tensegrity
Discover the role of fascia, tissue gliding, and invisible tension patterns in chronic pain. -
Bioactive Seating and Functional Rehabilitation
Learn how bioactive seating systems may support movement variability, postural adaptability, and long-term sitting comfort.
Sources and References
- Caneiro, J. P., O’Sullivan, P., Burnett, A., et al. (2021) — Reconceptualising pain and movement in musculoskeletal pain: implications for physical therapy. British Journal of Sports Medicine, 55(7), 387-394.
- Hartvigsen, J., Hancock, M. J., Kongsted, A., et al. (2018) — What low back pain is and why we need to pay attention. The Lancet, 391(10137), 2356-2367.
- World Health Organization (2023) — WHO guideline for non-surgical management of chronic primary low back pain in adults in primary and community care settings.
- NICE Guideline NG59 (2016, updated) — Low back pain and sciatica in over 16s: assessment and management. National Institute for Health and Care Excellence.
- Schleip, R., & Müller, D. G. (2013) — Training principles for fascial tissues: Scientific foundation and suggested practical applications. Journal of Bodywork and Movement Therapies, 17(1), 103-115.
- Van Dieën, J. H., De Looze, M. P., & Hermans, V. (2001) — Analysis of postural switching in sitting as a measure of comfort. Clinical Biomechanics, 16(8), 636-644.
- Panjabi, M. M. (1992) — The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. Journal of Spinal Disorders, 5(4), 383-389.