

Body Dynamics & Adaptability
Blue Portance Insights
Chronic Pain Decoded: Understanding the Invisible Mechanisms to Finally Take Action
Pain despite normal test results? Discover why your nervous system amplifies pain — and how to restore balance.
By Gil Ayache, PhD — Mines Paris – PSL · co-founder of Blue Portance
April 10, 2026
Summary — Chronic pain is not always a sign of tissue damage. It can result from a nervous system that has become hypersensitive: it amplifies signals, “learns” pain, and maintains an alert state even in the absence of any real threat. This mechanism — central sensitization — is biological, measurable, and above all, reversible. This article explains how it develops, what role fascia and mechanical constraints play, and why reintroducing movement variability is the key to recalibrating the system.
Introduction: A Puzzling Paradox
You experience persistent pain — sometimes intense, sometimes dull. Yet medical tests — MRI scans, X-rays, blood work — reveal no visible injury. Standard treatments provide little or no relief. And one question haunts you: “If everything looks fine… why am I in pain?”
This scenario, as frustrating as it is, is far more common than most people realize. An estimated 20% of adults in the US live with chronic pain without an identifiable organic cause. And no — it is not “all in your head.” The answer lies in a poorly understood biological mechanism: nervous system hypersensitization.
Before diving into the mechanisms, let’s set the framework: chronic pain can evolve along two distinct stages, depending on how the nervous system responds.
| Criterion | Stage 1 — Amplification | Stage 2 — Self-Sustaining |
|---|---|---|
| Cause | Real (injury, mechanical constraint) | Unidentifiable or secondary |
| Mechanism | Signal amplification | Autonomous signal production |
| System state | Hyper-reactive | Self-sustaining |
| Metaphor | Speaker turned up too loud | Scratched record / program stuck on loop |
| Therapeutic goal | Reduce sensitivity | Reprogram the system |
👉 This article focuses on Stage 1, where pain persists because the nervous system amplifies a signal that is still present.
1. Pain ≠ Injury: Breaking a Persistent Myth
1.1. The traditional model… and its limits
For decades, medicine has consistently equated pain = injury. This model, inherited from Descartes, assumes that:
- An injury or inflammation activates pain receptors (nociceptors).
- The signal travels up to the brain via the spinal cord.
- The brain interprets this signal as pain.
This framework fails to explain cases where pain persists without an underlying injury, or after that injury has healed.
- Chronic low back pain — 85% of MRI scans show no structural abnormality (Jensen et al., 1994).
- Fibromyalgia, where pain is diffuse and no detectable inflammation is present.
- Post-surgical pain that persists for months after complete healing.
1.2. The neuroscience revolution: central sensitization
In the 2000s, researchers such as Clifford Woolf (2011) demonstrated that the nervous system can become hypersensitive in response to repeated or prolonged stimuli. This phenomenon — central sensitization — is characterized by:
- A lowered pain threshold (allodynia: a light touch becomes painful).
- An amplified response (hyperalgesia: a pinprick is perceived as a burn).
- The spread of pain beyond the initial area.
“Chronic pain is not the symptom of a problem — it is the problem itself.” — Lorimer Moseley, neuroscientist and pain specialist (2012)
2. How Does the Nervous System Spiral Out of Control?
2.1. The brain in “maximum alert” mode
The nervous system is not a simple electrical wire — it is an adaptive network. When subjected to repeated, intense, or stress-associated pain signals, it activates exaggerated protective mechanisms.
- The amygdala — the region linked to fear and emotional memory — reinforces pain anticipation (Vachon-Presseau et al., 2016). A simple thought like “If I move, it’s going to hurt” can trigger a physical reaction.
- The somatosensory cortex expands to include healthy zones, as if the brain were “mapping” pain onto undamaged territories (Flor et al., 1995).
2.2. Neural plasticity: when pain is “learned”
The brain is plastic: it continuously remodels itself based on experience. In the context of chronic pain:
- Synapses strengthen, creating pain circuits that are more efficient… and harder to deactivate (Ji et al., 2003).
- NMDA receptors become hyperexcitable — like a switch stuck in the “ON” position (Latremoliere & Woolf, 2009).
“The nervous system does not lie. It exaggerates — but that’s to protect us. The problem is when it stays locked in protection mode.” — David Butler, physiotherapist, co-founder of the Neuro Orthopaedic Institute
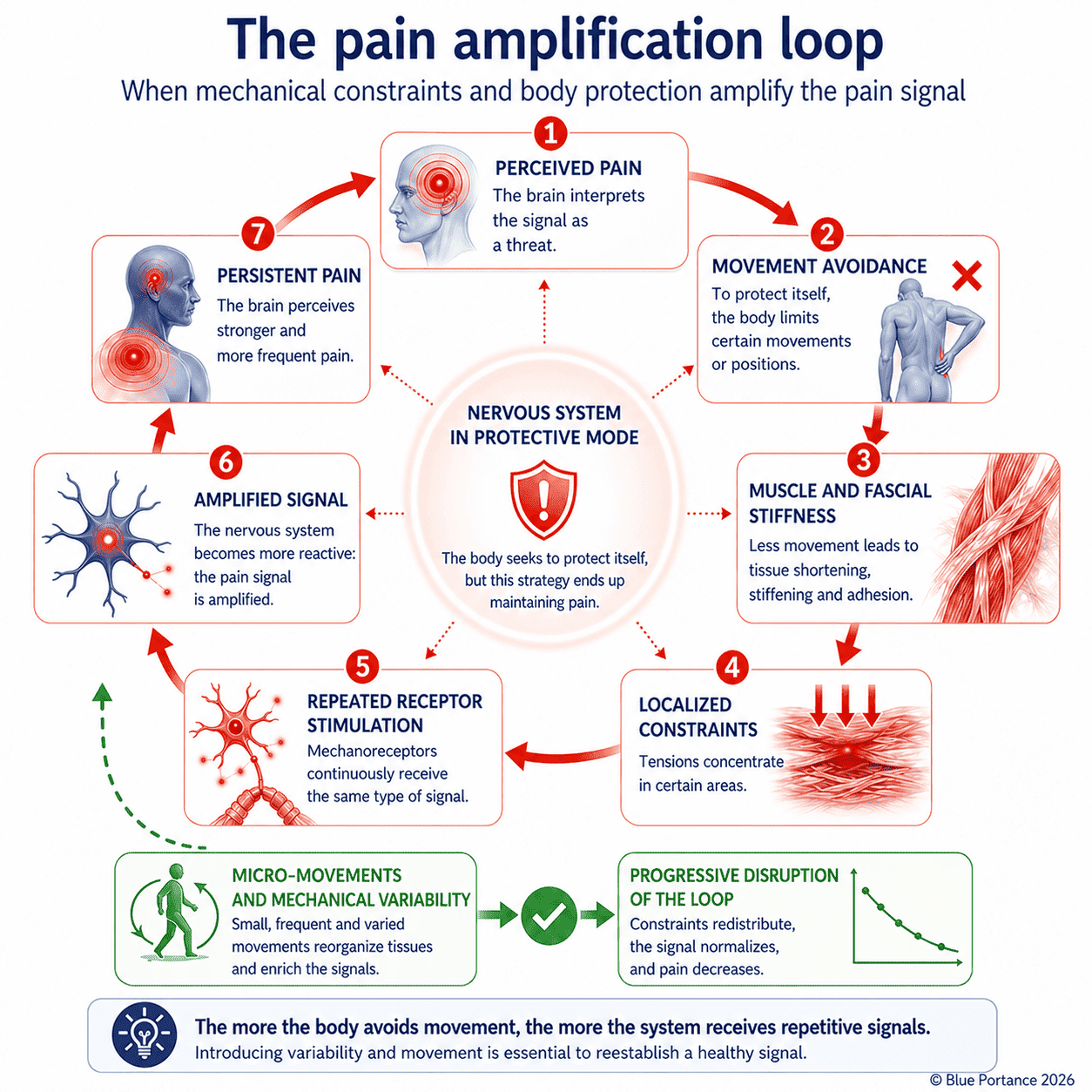
2.3. The amplification loop: pain → avoidance → pain
A vicious cycle takes hold:
- Pain → The patient avoids certain movements.
- Avoidance → Muscles and joints stiffen; fascia loses its gliding capacity.
- Stiffness → Mechanical constraints concentrate locally, stimulating nociceptors further.
- New pain signals → The nervous system amplifies them… and the loop reinforces itself.
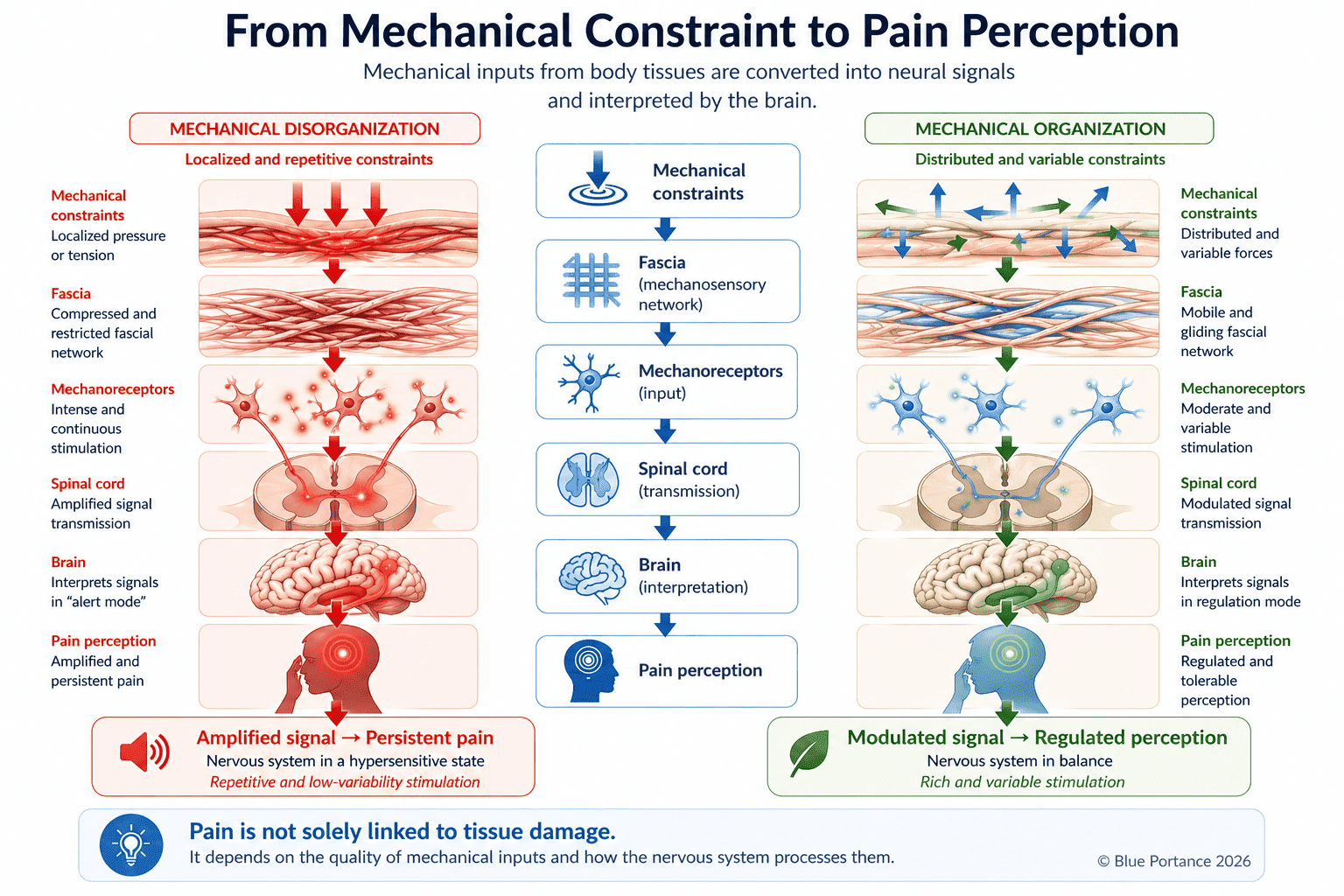
The nervous system does not create pain on its own: it reacts to a flow of mechanical information that can itself be disorganized. When constraints are localized, repetitive, and low in variability, they maintain continuous stimulation of sensory receptors — particularly within the fascia.
3. Why This Understanding Is Liberating
3.1. It’s not “psychological”… but it is modifiable
Chronic pain is not a product of the imagination. Functional MRI scans show real brain activation in pain-related areas (Apkarian et al., 2005).
This means:
- ✅ Your pain is biologically real, even without a visible injury
- ✅ It can be measured objectively through specialized testing
- ✅ It is not a sign of weakness or an imaginary problem
- ✅ And above all: it is potentially reversible, thanks to neuroplasticity
3.2. Neuroplasticity: the biological source of hope
The same mechanism that allows the brain to “learn” pain also enables it to unlearn it. Studies show that targeted interventions can:
- Reduce amygdala hyperactivity (mindfulness, relaxation techniques).
- Strengthen inhibitory circuits (progressive exercise, neuroscience-informed physiotherapy).
- Restore a normal body map in the somatosensory cortex (graded exposure therapy).
But neuroplasticity alone is not enough. To sustainably recalibrate the nervous system, we must also act on what continuously feeds it: mechanical constraints and the fascial network.
4. The Overlooked Role of Fascia in Chronic Pain
Fascia — the connective tissue that surrounds muscles, bones, and organs — forms a network that is both mechanical and sensory. Richly supplied with mechanoreceptors, fascia continuously transmits information to the nervous system about tensions, pressures, and tissue deformations (Schleip et al., 2012; Langevin, 2006).
When fascia is subjected to constraints that are:
- Continuous (prolonged static postures),
- Localized (zones of pressure or tension),
- Low in variability (lack of movement),
→ It loses its gliding capacity and sends “aberrant” signals to the nervous system (Langevin, 2006).
These signals may become decoupled from the actual mechanical state of the tissues — not because they are “false,” but because they reflect a system where constraints are poorly distributed and insufficiently varied. The nervous system then interprets them as a persistent threat, helping to maintain or amplify hypersensitization.
A patient with chronic neck pain may experience progressive stiffening of the fascia in the neck and shoulders. Constraints are no longer properly redistributed — they concentrate in certain areas, increasing stimulation of sensory receptors. By reintroducing variability — through progressive mobilization and micro-movements — it becomes possible to restore better constraint distribution and modulate the signals transmitted to the nervous system.
Stage 1 chronic pain rests on a mechano-neural loop: fascial constraints feed hypersensitization, which in turn amplifies the perception of those constraints. Acting on one means acting on the other.
5. How to “Unlearn” Pain?
5.1. Reintroducing movement through continuous micro-adjustments
Unlearning pain is not simply about “moving more.” The essential point is to reintroduce gentle, frequent, non-threatening movements capable of progressively modifying the information transmitted to the nervous system.
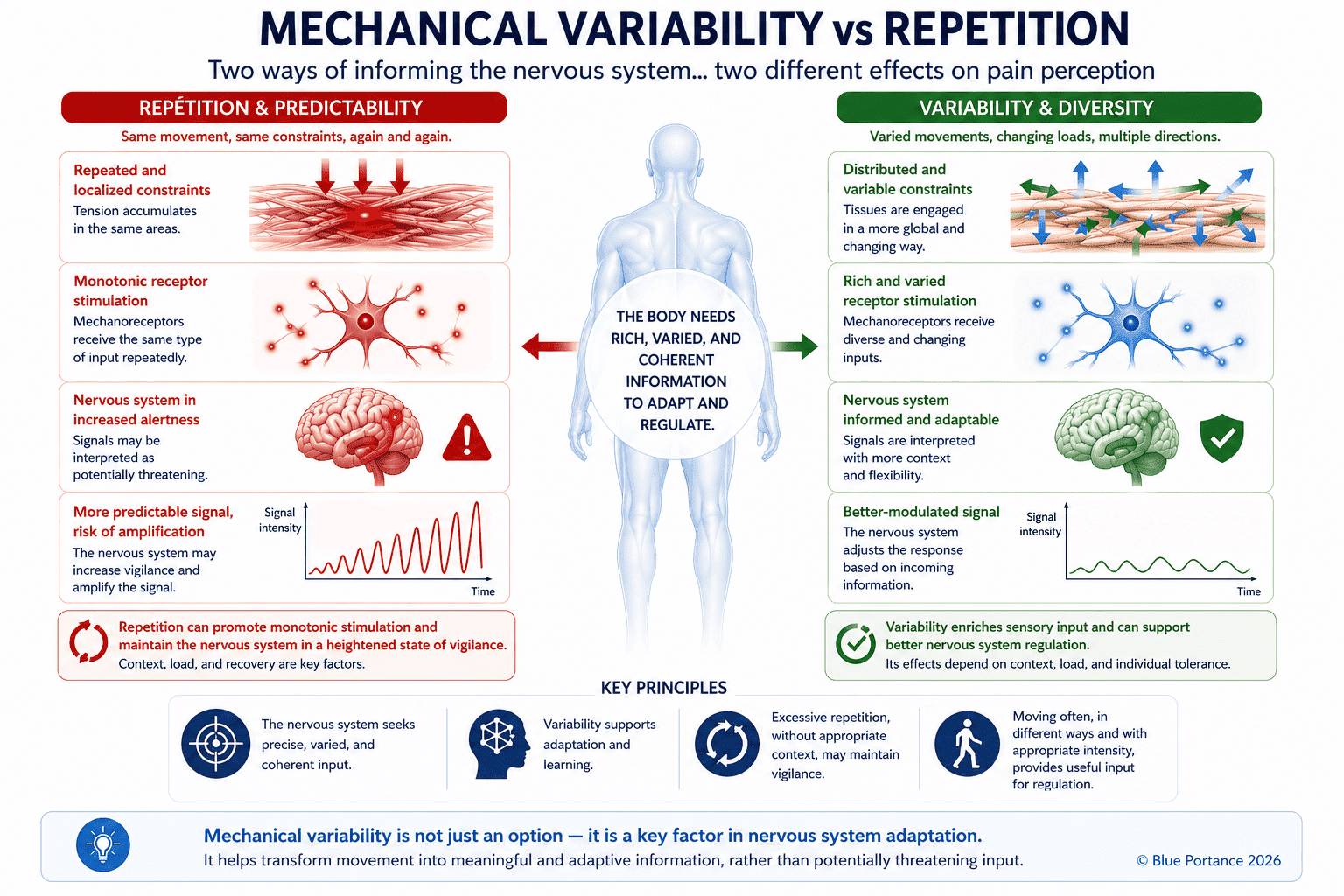
Micro-movements — breathing, gentle pelvic tilts, postural adjustments, shifts in weight — recreate mechanical variability. This variability helps tissues distribute constraints more evenly, promotes fascial gliding, and enriches the sensory signals sent to the brain.
The nervous system then receives less repetitive, less alarming information — and can progressively reduce its level of hypervigilance.
To explore this mechanism further: Why Micro-Movement Matters More Than Moving A Lot
5.2. Addressing beliefs and fear of movement
Fear of pain (kinesiophobia) often worsens the problem:
- Patients who fear movement are twice as likely to develop chronic pain (Vlaeyen & Linton, 2000).
- Pain neuroscience education reduces anxiety and improves mobility (Moseley et al., 2004).
- Pain journal: log triggering situations and associated thoughts.
- Mindfulness meditation: observe pain without judgment — shown to reduce pain intensity by approximately 20% (Kabat-Zinn, 1985).
5.3. Diet and silent inflammation
Certain pro-inflammatory foods (refined sugar, trans fatty acids) can further sensitize the nervous system. Conversely:
- Omega-3 fatty acids (fatty fish, walnuts) reduce neurogenic inflammation (Calder, 2017).
- Curcumin modulates NMDA receptor response (Wang et al., 2010).
5.4. When to seek professional help?
If your pain persists for more than 3 months despite your efforts, spreads to other areas of the body, or becomes unpredictable (appearing without a clear trigger), it is possible that you have reached Stage 2 — where the nervous system generates pain autonomously.
👉 In that case, read our companion article:
Part 2: “When Pain Becomes Autonomous — Neurosensory Reprogramming”
- Why pain can persist without any mechanical cause
- How the nervous system generates phantom signals
- Specific strategies to rewire the brain (mirror therapy, neurofeedback…)
➡️ Read Part 2
Key Takeaways: 5 Essential Ideas
- Chronic pain ≠ injury — it is often a nervous system dysfunction, not a wound.
- The brain can “learn” pain — through neural plasticity, circuits strengthen… but can also be deactivated.
- The amygdala and fear play a central role — pain is also an emotional experience.
- Fascia is an underappreciated player — its state directly influences the transmission of pain signals.
- The solution lies in rehabilitation — progressive movement, variability, and stress management are the keys to recalibrating the system.
Analyze Your Pain to Find the Right Solution
If you recognize yourself in these mechanisms — pain while sitting, persistent discomfort, or a feeling of stiffness — the next step is to identify what is mechanically sustaining these constraints.
The real question becomes simple: does your seat still allow your body to function freely… or is it gradually preventing it from doing so?
👉 Our personalized analysis tool identifies the specific mechanisms involved in your seated pain — and helps you find the Aporia® version best suited to your situation.
Analyze my pain and find the right Aporia® version for my situationFrequently Asked Questions
What is central sensitization?
Why am I in pain when my MRI is normal?
What is the connection between fascia and chronic pain?
Why do micro-movements help reduce pain?
How do I know whether I’m at Stage 1 or Stage 2?
Further Reading
Explore on Blue Portance
- ➡️ Chronic Pain Part 2: When Pain Becomes Autonomous — Neurosensory Reprogramming
- ➡️ The overlooked role of fascia: Fascia and Tensegrity Explained: How Your Body Regulates Mechanical Stress, Movement, and Pain
- ➡️ The importance of micro-movements: Why Micro-Movement Matters More Than Moving A Lot
Scientific References
- Woolf, C. J. (2011). Central sensitization: Implications for the diagnosis and treatment of pain. Pain, 152(3 Suppl), S2–S15. [PubMed]
- Moseley, G. L. (2012). Reconceptualising pain according to modern pain science. Physical Therapy Reviews, 17(3), 169–178. [PubMed]
- Latremoliere, A., & Woolf, C. J. (2009). Central sensitization: A generator of pain hypersensitivity by central neural plasticity. Journal of Pain, 10(9), 895–926. [PMC]
- Langevin, H. M. (2006). Connective tissue: A body-wide signaling network? Medical Hypotheses, 66(6), 1074–1077. [PubMed]
- Schleip, R., et al. (2012). Fascia as a sensory organ. Fascia: The Tensional Network of the Human Body. Churchill Livingstone / Elsevier. [Source]
- Vachon-Presseau, E., et al. (2016). The emotional brain as a predictor and amplifier of chronic pain. Journal of Dental Research, 95(6), 605–612.
- Vlaeyen, J. W. S., & Linton, S. J. (2000). Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain, 85(3), 317–332. [PubMed]
- Apkarian, A. V., et al. (2005). Chronic back pain is associated with decreased prefrontal and thalamic gray matter density. Journal of Neuroscience, 25(45), 10410–10415. [PubMed]
“Pain is inevitable, suffering is optional.” — Buddhist proverb (adapted to neuroscience)
© Blue Portance. Reproduction and distribution authorized for non-commercial purposes, provided the source is cited: “Blue Portance – SBNFA™ Doctrine”.