

Body Dynamics & Adaptability
Blue Portance Insights
Chronic Pain Decoded: Understanding the Invisible Mechanisms to Finally Take Action
Pain that appears without a trigger, migrates, or persists at rest despite normal test results? Understand why the nervous system can produce pain autonomously — and how to reprogram it.
Summary — In 10 to 30% of chronic pain cases, a critical threshold is crossed: the nervous system no longer merely amplifies pain signals — it produces them autonomously. Pain appears without any identifiable trigger, persists at rest, and may migrate. This mechanism — neurosensory disruption — rests on a maladaptive learning process in the brain and spinal cord. It is not irreversible: the same neuroplasticity that installed the pain can help undo it. This article explains the mechanisms of Stage 2 and the concrete strategies available to reprogram the system.
Introduction: The Stage Where Everything Shifts
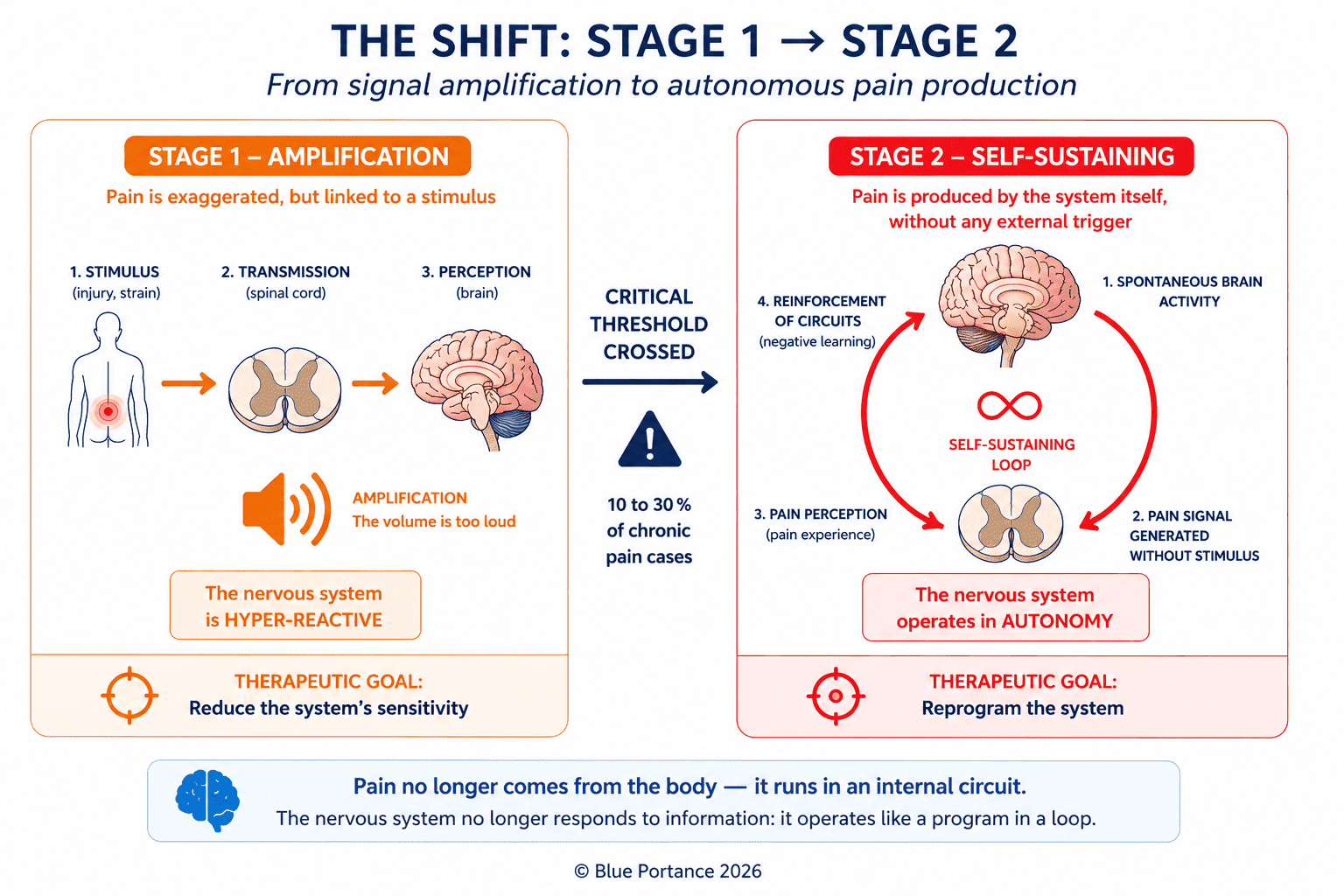
In Part 1, we saw how the nervous system can become hypersensitized: it amplifies pain signals, like a speaker turned up too loud. But in 10 to 30% of chronic pain cases (Apkarian et al., 2021), a critical threshold is crossed — pain no longer follows the logic of “stimulus → reaction.”
As a result, it appears spontaneously, persists at rest, or migrates without any mechanical explanation.
This is Stage 2: neurosensory disruption.
The nervous system is no longer responding to information — it functions as a self-organizing system capable of producing its own pain activity.
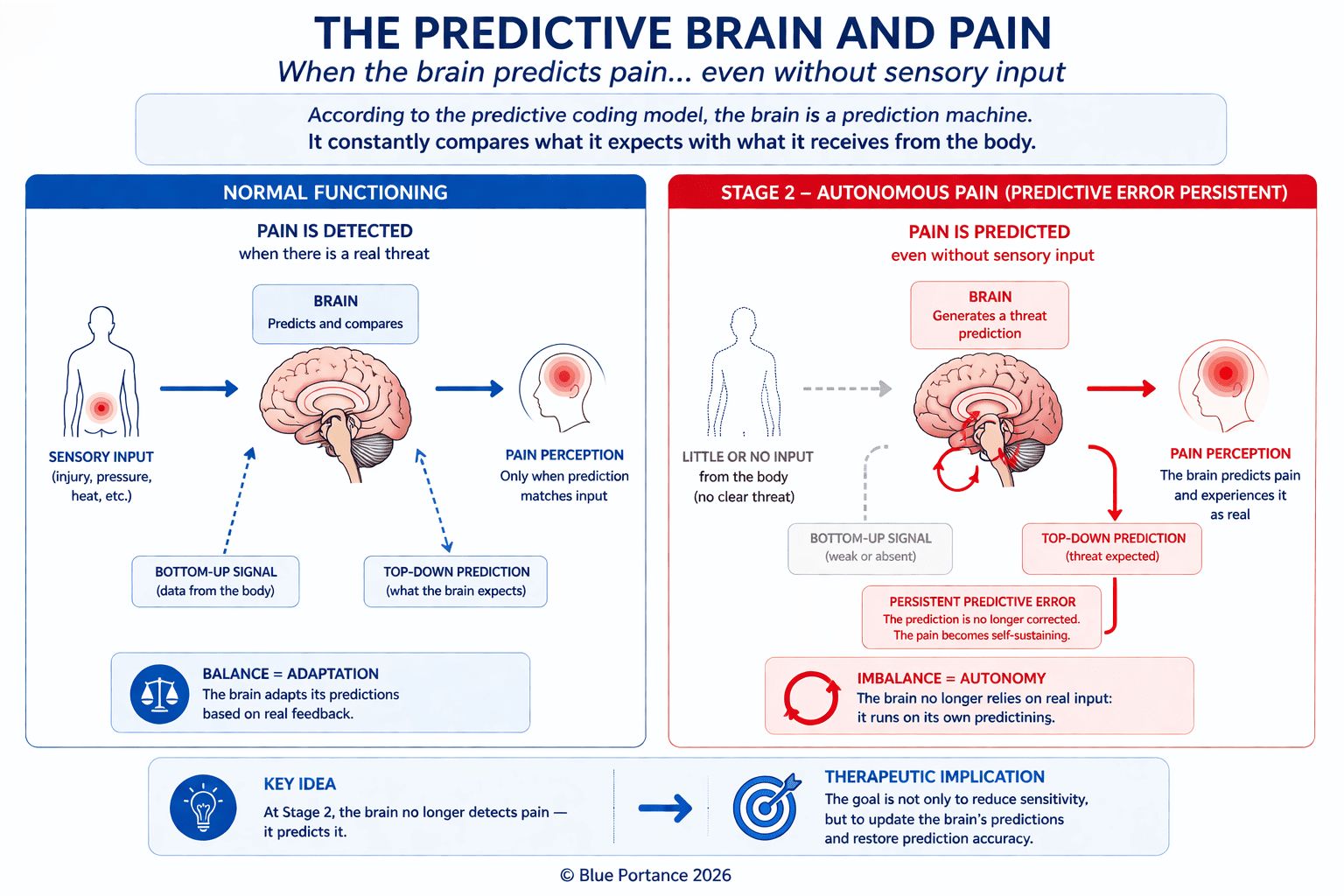
This shift corresponds to a transition from a reactive system to an autonomous predictive system, in which the brain generates perceptual hypotheses independently of sensory input (Friston, 2010; Edwards et al., 2012).
1. The Break: When Pain Detaches from Mechanical Reality
1.1. The defining feature of Stage 2
Unlike Stage 1 (where pain is exaggerated but linked to a stimulus), at Stage 2:
First, there is no identifiable trigger: pain arises without movement, without pressure, sometimes even at night. Second, a temporal decoupling develops: it can persist for months after complete healing of an injury. Finally, an unexplained migration may occur: pain shifts location without mechanical cause — for instance, moving from one arm to the other.
“At Stage 2, the nervous system is no longer processing information — it is generating it.” — Vania Apkarian, Nature Reviews Neuroscience (2016)
1.2. Predictive coding: the brain anticipating pain
Indeed, this phenomenon falls within the framework of predictive coding: the brain no longer simply processes sensory signals — it anticipates and generates perceptions based on internal models built through experience.
Consequently, pain becomes a dominant prediction, maintained even in the absence of peripheral confirmation (Clark, 2013; Büchel et al., 2014).
1.3. Scientific evidence for system autonomy
The scientific evidence is converging on several fronts. First, functional MRI reveals spontaneous cerebral activation in pain areas — specifically the somatosensory cortex and insula — even in the absence of any stimulation (Baliki et al., 2012). Furthermore, at the spinal cord level, certain neurons in the dorsal horn can self-activate after prolonged sensitization, producing a state of spinal network hyperexcitability (Latremoliere & Woolf, 2009). Perhaps most striking is the case of phantom limb pain: amputees experience real pain even though there are no longer any nerves to transmit it (Flor et al., 2006).
2. The Mechanisms of Neurosensory Disruption
2.1. The spinal cord in “generator mode”
At Stage 1, the spinal cord amplifies signals. At Stage 2, it produces them:
First, the “wind-up” phenomenon occurs: a single stimulation triggers a prolonged response — like an echo that never stops. Furthermore, certain neurons become hyperexcitable and discharge spontaneously, even without peripheral input (Woolf, 2011). Finally, and perhaps most critically, inhibitory mechanisms weaken: GABAergic interneurons, which normally suppress pain, become progressively deficient (Zeilhofer et al., 2012).
2.2. The brain: from amplification to generation
Moreover, three brain regions play a specific role at Stage 2:
| Brain region | Role at Stage 1 | Role at Stage 2 | Reference |
|---|---|---|---|
| Amygdala | Amplifies fear of pain | Generates anticipatory pain | Vachon-Presseau et al., 2016 |
| Prefrontal cortex | Moderates perception | Loses its capacity to inhibit pain | Lorenz et al., 2003 |
| Hippocampus | Stores the pain experience | Recreates pain as a memory | Apkarian et al., 2009 |
In other words, the brain no longer “reacts” to pain: it integrates it into its baseline functioning, via a reconfiguration of the Default Mode Network (Baliki et al., 2008).
For example, a patient who hurt their back lifting a heavy object can, years later, feel pain simply by watching someone else pick up a box. This is an associative generalization mechanism: neutral stimuli activate the memory and emotional networks linked to pain (Apkarian et al., 2011).
2.3. The body: involuntarily feeding the loop
However, even when the system has become autonomous, the body continues to fuel the loop through three channels:
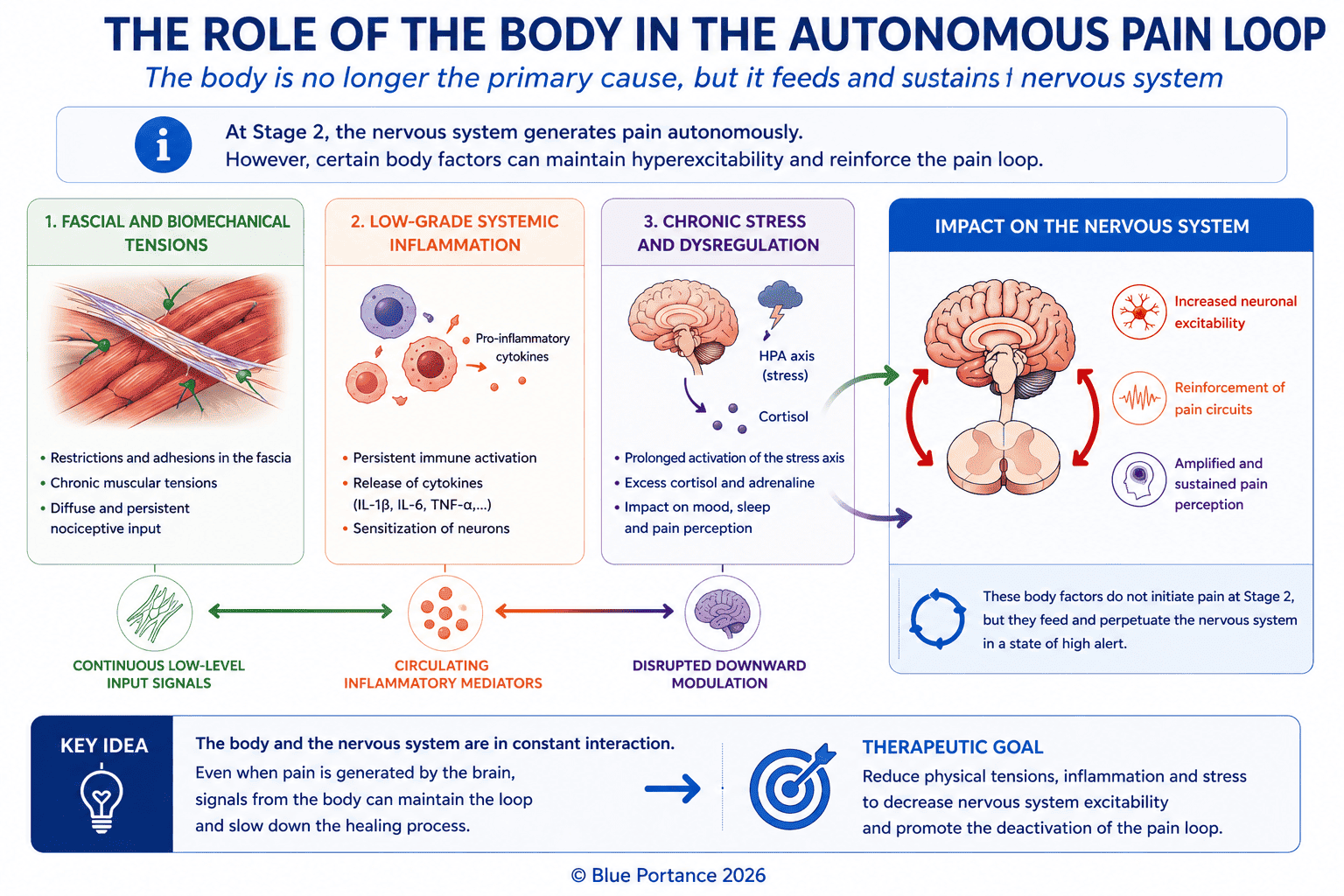
- Chronically tense fascia sends constant pressure signals to the nerves (Langevin, 2006). A stiff thoracic fascia can compress intercostal nerves, sustaining a pain signal.
- The immune system — even low-grade inflammation, undetectable in standard blood tests, can sensitize spinal cord neurons (Grace et al., 2016).
- The endocrine system — excess cortisol increases neuronal excitability (McEwen, 2003).
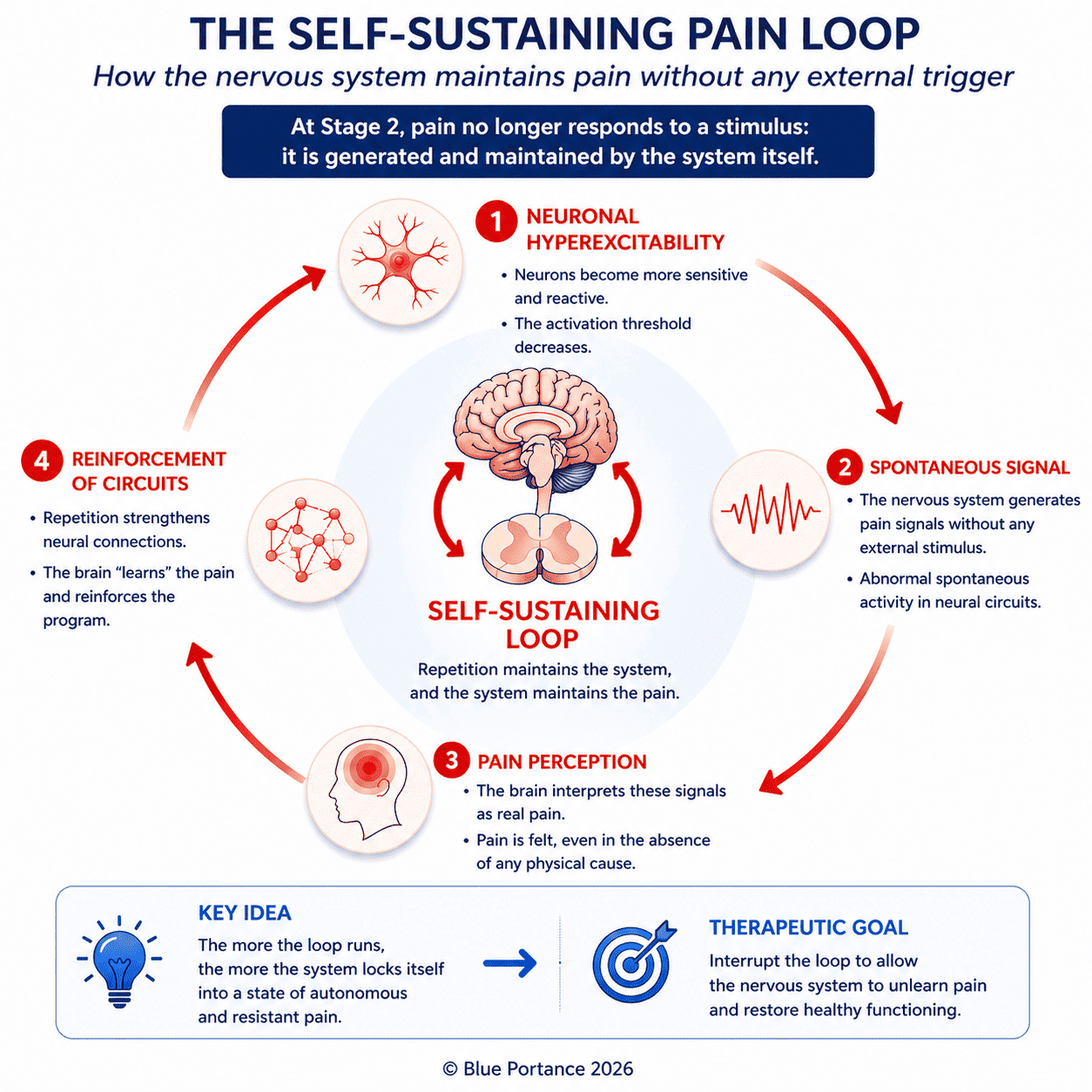
2.4. Perpetuation: why the loop locks itself in
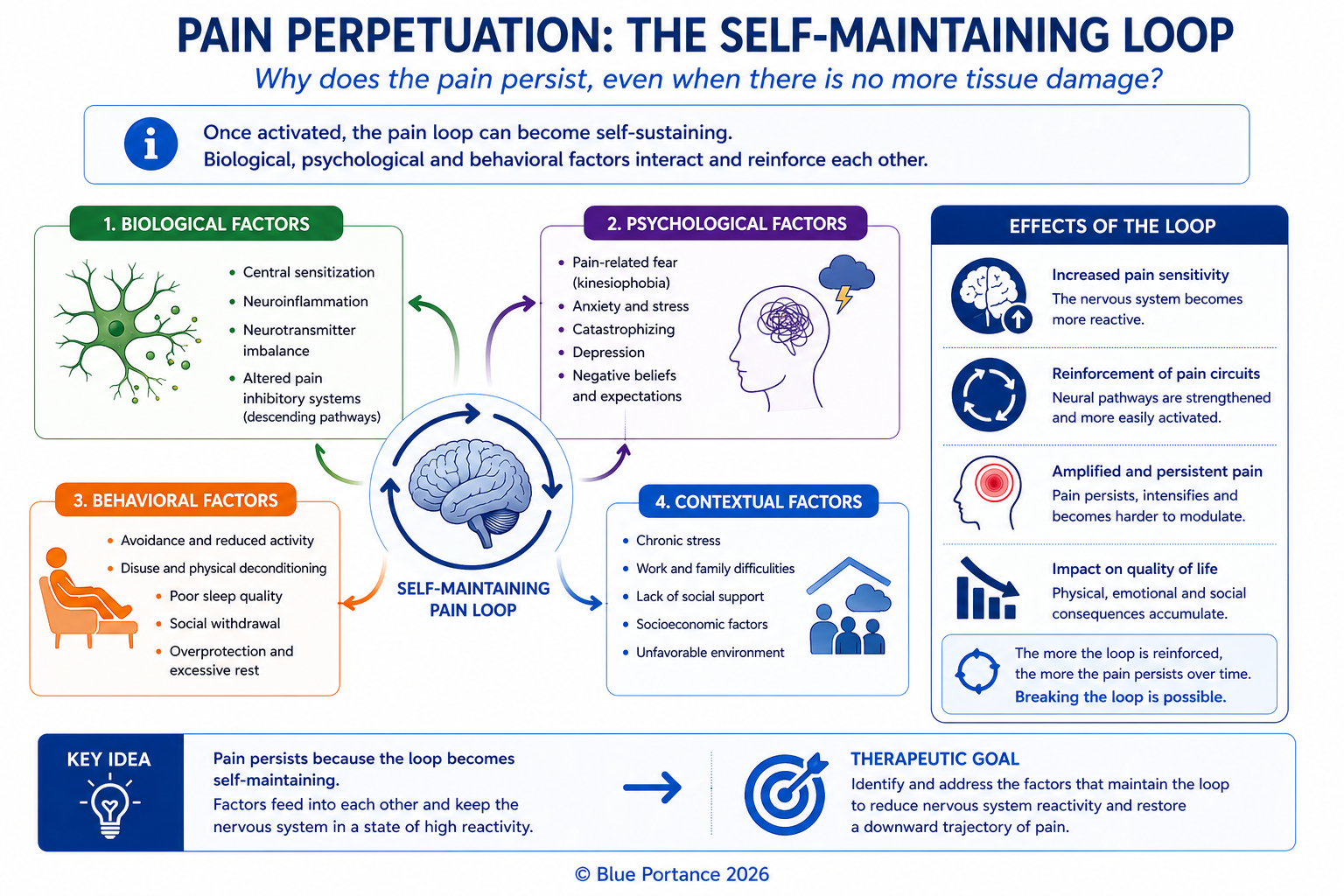
At Stage 2, pain rests on a system driven by autonomous neurocentral control, reinforced by adaptive stabilization of circuits and sustained by an integrated memory of the pain signal.
👉 As a result, pain is no longer an alarm. It becomes an emergent property of the nervous system itself.
3. The Challenge of Neurosensory Reprogramming
At this stage, the goal is no longer to treat a painful zone — it is to reprogram an autonomous nervous system. The challenge is no longer local: it is systemic — breaking a biological automatism.
3.1. Why “reprogramming” and not “deprogramming”?
Therefore, the objective is not to erase pain circuits, but to teach them how to function normally again (Friston, 2010; Edwards et al., 2012). As Apkarian et al. (2016) demonstrate, the brain has learned to generate pain — and it can therefore unlearn this habit. Specifically, this happens through synaptic plasticity — strengthening new circuits — as well as through descending modulation to restore inhibitory mechanisms, and ultimately through sensorimotor rewiring via mirror therapy and motor imagery.
3.2. The three levers of reprogramming
- First,the principle of non-pain — any painful stimulation validates the nervous system’s prediction and reinforces the loop. Reprogramming must be done strictly below the pain threshold to avoid reactivating the amygdala.
- Second, saturation with safety signals — flooding the spinal cord and brain with neutral or pleasant sensory information. By multiplying micro-movements, thermal stimulations, and gentle pressures, the ratio of painful to safe signals is progressively shifted.
- Finally, restoring body maps — giving “definition” back to the brain’s blurry zones. By using vision (mirror) and focused attention, the system is pushed to recreate a precise image of the body — rendering phantom signals obsolete.
Indeed, fibromyalgia patients perfectly illustrate this mechanism: diffuse pain without identifiable injury, allodynia (pain from the lightest touch), and central fatigue linked to neuronal hyperexcitability. Neurosensory reprogramming protocols (Moseley & Flor, 2012) deliver significant symptom reduction in 8 to 12 weeks, where standard approaches fail.
Together, these three levers define the therapeutic framework. The next step is translating them into concrete interventions capable of influencing the nervous system at multiple levels simultaneously.
4. Implementing Reprogramming: Progressive Strategies
4.1. Stay below the pain threshold
Goal: avoid any reactivation of the alert system and prevent reinforcement of the autonomous loop.
The 80% rule:
For instance, if a movement becomes painful at 90° of range of motion, limit to 72°. Any painful stimulation confirms the nervous system’s prediction (“this movement = danger“) and reinforces the circuit via the amygdala (Vachon-Presseau et al., 2016).
→ Reprogramming must be performed at 80% of the maximum pain threshold.
4.2. Saturate with safety signals
Goal: reduce hyperexcitability by modifying sensory input.
- Transcutaneous electrical nerve stimulation (TENS) — high frequency (50–100 Hz) activates A-beta fibers (non-painful), which inhibit C fibers (pain) via gate control theory (Melzack & Wall, 1965). Protocol: 20 min/day at sub-threshold intensity.
- Contrast bath (hot/cold) — alternation resets thermal receptors, disrupting automatic signals (Bleakley & Davison, 2010). Example: 1 min cold water (50–59°F) → 1 min warm water (100–104°F), repeated 5 times.
- Micro-movements and gentle mobilization — a constant flow of non-painful proprioceptive information without triggering a defensive response. For instance, very slow ankle circles within a pain-free range.
4.3. Restore cortical maps
Goal: correct distortions in body representation and reduce predictive pain signals.
Additionally, at Stage 2, the somatosensory cortex often shows overrepresentation of painful zones (distorted map) and a loss of precision in sensation localization:
Healthy brain: [Hand] → Normal area in the cortex Stage 2: [Hand] → Enlarged and blurry area After reprogramming: [Hand] → Redrawn area
-
Mirror therapy — the brain “sees” a pain-free movement and rewires the motor representation (Ramachandran & Rogers-Ramachandran, 1996).
Protocol:
- 5 min of symmetrical movements (e.g., opening/closing the hands)
- 3 sessions per day, progressively increasing complexity
- Move to asymmetrical movements after 2 weeks
Expected result: 30–40% pain reduction in 4–6 weeks (Moseley et al., 2008).
-
Graded motor imagery (GMI) — reactivate cortical zones without actual movement.
- Phase 1: imagine the movement (e.g., raising an arm) for 2 min
- Phase 2: perform the movement, twice as slowly as normal
- Phase 3: progressively increase speed over 4–6 weeks
Particularly effective for complex regional pain syndrome (CRPS) (Bowering et al., 2013).
- Neurofeedback — use EEG to visualize pain-related brain activity and learn to modulate it. Sessions of 30 min, 2–3 times/week. 40% reduction in pain intensity in fibromyalgia patients (Kayiran et al., 2010).
4.4. Cut off peripheral fuel sources
Goal: reduce the body signals that sustain hyperexcitability.
| Healthy fascia | Fascia at Stage 2 | Impact on pain |
|---|---|---|
| Fluid gliding between layers | Adhesions and restrictions | Mechanoreceptor compression → aberrant signals |
| Normal hydration | Dehydration (lack of movement) | Stiffness → continuous nerve stimulation |
| Even constraint distribution | Localized tension zones | Overloading of certain areas → pain loop |
Fascia strategy:
- Foam roller self-massage: 2–3 min per area, without pain. Prioritize zones adjacent to the pain (e.g., thighs for low back pain).
- Hydration: 1.5–2 L of water/day + omega-3 to restore tissue elasticity. Avoid pro-inflammatory foods (refined sugar, trans fats).
- Spiral movements: arm circles, hip rotations to restore variability — 3 sets of 10 movements in each direction, 2×/day. Strictly avoid aggressive passive stretching or painful pressure.
5. Case Study: Sophie’s Protocol
Context
Note: this is an illustrative composite case, reconstructed from clinically documented mechanisms.
Sophie, 42, has suffered from chronic pelvic pain for 5 years. All tests (MRI, ultrasound, blood work) are normal. She has tried physiotherapy, osteopathy, antidepressants… without success.
Diagnosis: Stage 2 neurosensory disruption — autonomous pain + emotional memory linked to a traumatic childbirth.
| Week | Action | Result |
|---|---|---|
| 1–2 | Mirror therapy (10 min/day) + TENS | 20% reduction in intensity |
| 3–4 | Graded motor imagery + fascia release (foam roller) | Pain less frequent |
| 5–8 | Neurofeedback (2×/week) + diaphragmatic breathing | 50% pain reduction |
| 9–12 | Progressive movement reintroduction (gentle yoga) | Occasional, manageable pain |
Above all, combining multiple approaches to act on all levels simultaneously — spinal cord, brain, and body — was the key to success. No single approach in isolation would have been sufficient to break the loop.
Summary: Stage 1 vs Stage 2
| Criterion | Stage 1 — Hypersensitization | Stage 2 — Neurosensory Disruption |
|---|---|---|
| Mechanism | Signal amplification | Autonomous signal generation |
| Trigger | Mechanical stimulus (movement, pressure) | None or emotional memory |
| Location | Specific zone | Possible migration |
| Key treatment | Stimulus reduction + stress management | Neurosensory rehabilitation (spinal cord + brain) |
| Typical example | Low back pain after a sudden movement | Phantom pain, fibromyalgia |
Apply These Principles to Your Daily Life
In practice, neurosensory reprogramming does not end in therapy sessions. It begins with the environment where you spend the most time — particularly in a seated position.
The real question becomes: does your seat allow your nervous system to receive continuous safety signals… or does it sustain the loop?
👉 Our personalized analysis tool identifies the mechanisms involved in your pain and helps you find the Aporia® version best suited to your situation.
Analyze my pain and find the right Aporia® version for my situationFrequently Asked Questions
What is neurosensory disruption?
How do I tell Stage 1 from Stage 2?
Is mirror therapy effective for all types of pain?
How long does it take to reprogram the nervous system?
Can these approaches be combined with standard medical treatment?
Further Reading
Explore on Blue Portance
- ➡️ Chronic Pain Part 1: Why Pain Persists When Everything Seems Normal — Hypersensitization
- ➡️ The overlooked role of fascia: Fascia and Tensegrity Explained: How Your Body Regulates Mechanical Stress, Movement, and Pain
- ➡️ The importance of micro-movements: Why Micro-Movement Matters More Than Moving A Lot
Practical resources
- App: PainScience — guided neuroplasticity exercises.
- Book: The Explain Pain Handbook: Protectometer (Butler & Moseley) — a practical guide to deactivating autonomous pain circuits.
- Professional training: certifications in mirror therapy and neurofeedback.
Scientific References
- Apkarian, A. V., et al. (2016). Pain and the brain: Specificity and plasticity of the brain in clinical pain states. Nature Reviews Neuroscience. [PubMed]
- Baliki, M. N., et al. (2012). Cortical thickness and functional connectivity in chronic back pain. Journal of Neuroscience, 32(33), 11344–11353. [PubMed]
- Bowering, K. J., et al. (2013). The effects of graded motor imagery and its components on chronic pain. Journal of Pain. [PubMed]
- Flor, H., et al. (2006). Phantom-limb pain: Characteristics, causes, and treatment. The Lancet Neurology, 5(8), 696–707. [PubMed]
- Friston, K. (2010). The free-energy principle: a rough guide to the brain? Nature Reviews Neuroscience. [PubMed]
- Kayiran, S., et al. (2010). Neurofeedback intervention in fibromyalgia syndrome. Applied Psychophysiology and Biofeedback. [PubMed]
- Langevin, H. M. (2006). Connective tissue: A body-wide signaling network? Medical Hypotheses. [PubMed]
Additional references
- Latremoliere, A., & Woolf, C. J. (2009). Central sensitization. Journal of Pain. [PMC]
- Melzack, R., & Wall, P. D. (1965). Pain mechanisms: A new theory. Science. [PubMed]
- Moseley, G. L., et al. (2008). Graded motor imagery for pathologic pain. Neurology. [PubMed]
- Moseley, G. L., & Flor, H. (2012). Targeting cortical representations in the treatment of chronic pain. Neurorehabilitation and Neural Repair. [PubMed]
- Ramachandran, V. S., & Rogers-Ramachandran, D. (1996). Synaesthesia in phantom limbs induced with mirrors. Proceedings of the Royal Society B. [PubMed]
- Woolf, C. J. (2011). Central sensitization. Pain. [PubMed]
- Zeilhofer, H. U. (2012). GABAergic inhibition in the spinal cord and its role in the control of pain. Neuroscience Letters, 520(2), 197–203.
“Stage 2 chronic pain is like a scratched record: the brain is stuck on a single melody. Our work is to teach it how to change the tune.” — David Butler
Putting it into practice: How to concretely integrate these neurosensory reprogramming principles into your daily life — especially while seated?
© Blue Portance. Reproduction and distribution authorized for non-commercial purposes, provided the source is cited: “Blue Portance – SBNFA™ Doctrine”.