

Your pain in a seated position may depend on your pelvi-spinal organization. Understanding your natural balance profile is a first step toward grasping what happens when you sit down.
Summary — Your pain in a seated position is not a matter of postural willpower. It is a problem of geometric compatibility between your morphology and your seat. Every individual has a unique pelvi-spinal organization — permanently fixed at puberty — that determines how their body tolerates, compensates for, or resists a given seating geometry.
The real challenge is therefore not to impose a universal posture, but to understand how the pelvis, femurs, and spine can recover a coherent relationship according to the subject’s natural profile.
The SBNFA™ doctrine proposes to restore these conditions of balance: respecting pelvic orientation, preserving freedom of micro-adjustment, and adapting the thigh-pelvis relationship rather than locking the body into a standardized posture.
Introduction
Why do some people develop pain after just a few minutes in a seated position, while others seem able to sit all day without any apparent difficulty?
At first glance, this might suggest that certain body types are better suited to sitting than others.
Yet research on the sagittal balance of the spine tells a different story.
Prolonged seated posture constitutes a biomechanical constraint for everyone.
The difference does not lie in the ability to withstand this constraint, but in the way each organism adapts to it: some compensate for longer, others reach their adaptive limits more quickly.
Understanding these differences requires attention to an often-overlooked element: spinal profiles, and the natural balance profile that flows from them for each individual.
1. Why we are not all built the same way
When we talk about seated posture, we tend to imagine that there is an ideal position applicable to everyone.
This seems logical. After all, if we all share the same skeleton, why couldn’t we all adopt the same posture? Yet the reality is more complex.
Research on sagittal spinal balance has shown that we are not all organized the same way from a pelvi-spinal standpoint — in other words, we do not all naturally seek our balance through the same biomechanical strategy.
In some individuals, the pelvis naturally tends toward a more posterior orientation; in others, it adopts a more vertical position; in others still, it spontaneously tilts forward.
These differences are not anomalies, nor signs of poor posture: they simply represent different ways the human body organizes its balance.
This natural pelvic orientation directly influences the organization of spinal curves, the position of the center of gravity, and the way mechanical constraints are distributed throughout the musculoskeletal system.
Thus, two people of the same height and weight may display very different pelvi-spinal organizations, yet be perfectly balanced in a standing position and remain asymptomatic.
But when confronted with the same seating geometry, their responses may differ greatly.
Understanding this diversity is an essential step, because before trying to explain why some people develop pain while seated, we must first recognize that they do not all start from the same balance point.
It is precisely this natural diversity that Pierre Roussouly’s work helped to describe more precisely through the concept of spinal profiles.
2. Roussouly’s spinal profiles
The seated position represents a major biomechanical challenge due to its impact on the sagittal balance of the spine and pelvis. Contrary to a persistent misconception, there is no universally correct seated posture — there are distinct pelvi-spinal organizations, each with its own natural balance point.
The work of Pierre Roussouly and his collaborators made it possible to identify and classify these profiles according to a key anatomical parameter: pelvic incidence (PI), defined as the angle between the perpendicular to the sacral endplate and the line connecting the center of the femoral heads to the center of the sacral endplate. This angle, unique to each individual and permanently fixed at puberty — around age 10–12, with the ossification of the pelvis and sacrum — directly conditions the organization of all the spinal curves above it.
2.1. Classification of sagittal profiles
This early fixation is fundamental: it means that PI is not an adopted posture, but a permanent bony structure. After puberty, no rehabilitation can modify it. The way the body organizes its balance in a seated position is inscribed in bone long before adulthood — and this is precisely what conventional ergonomic thinking ignores when it seeks to “correct” an individual’s posture toward an external norm.
Observed at an African market. A young girl carrying an exceptionally heavy crate on her head had her entire postural organization transform within seconds. The pelvis tilted forward, the lumbar lordosis dramatically increased, and the buttocks were projected backward to maintain the balance of the load. This genuine postural metamorphosis was a striking observation for me.
It immediately raised a question: when such constraints are repeated daily throughout the entire growth period, can they contribute to the construction of the adult’s sagittal profile?
Four main types are identified according to the value of pelvic incidence and the resulting spontaneous pelvic orientation (Roussouly & Pinheiro-Franco, 2011):
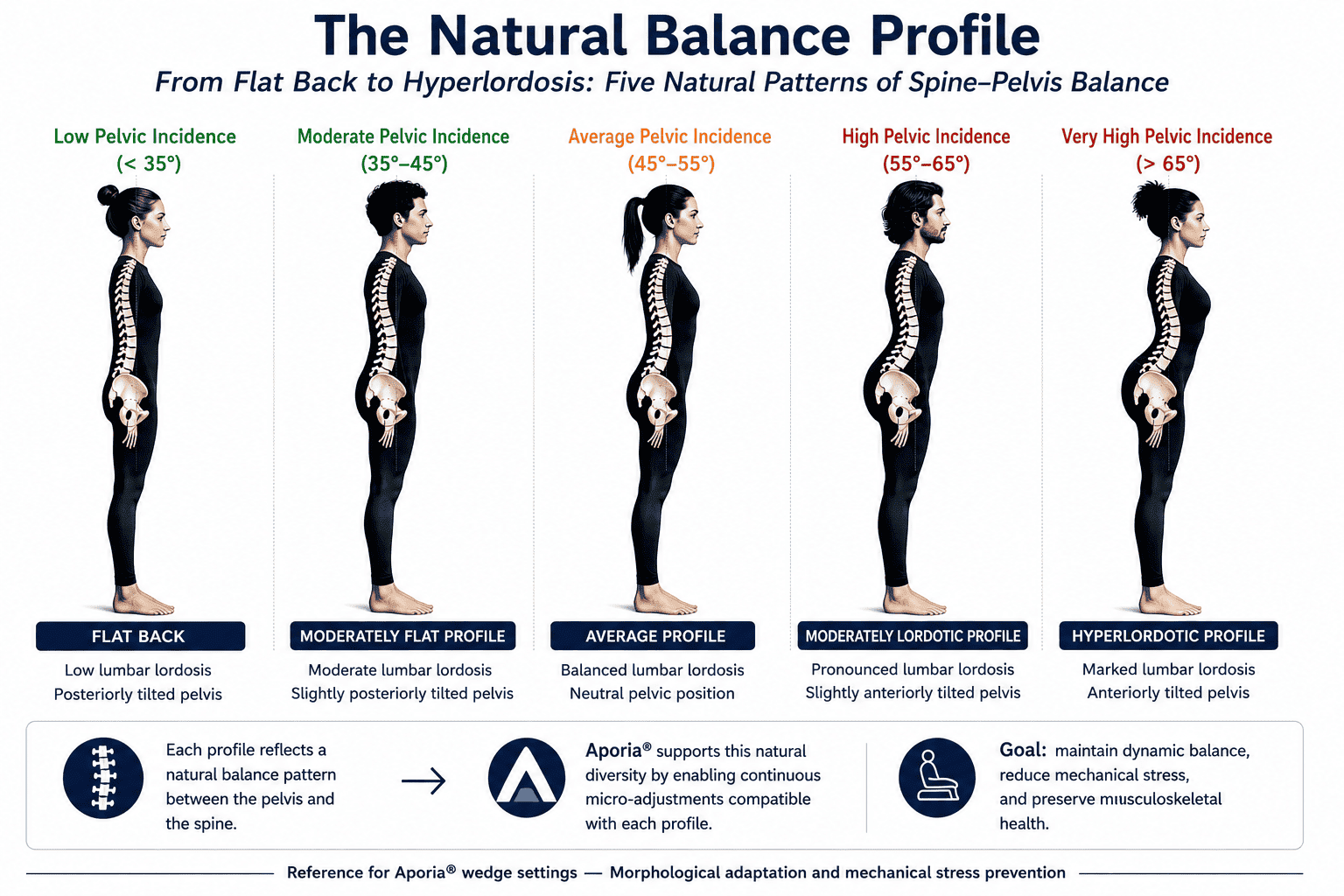
| Profile | Pelvic incidence | Natural pelvic orientation | Spinal characteristics |
|---|---|---|---|
| Type 1 | < 35° | Natural retroversion | Low lumbar lordosis, moderate thoracic kyphosis |
| Type 2 | 35°–55° | Vertical pelvis | Moderate lumbar lordosis, neutral sagittal balance |
| Type 3 | 55°–75° | Natural anteversion | Marked lumbar lordosis, low thoracic kyphosis |
| Type 4 | > 75° | Very marked anteversion | Very marked lumbar lordosis, absent thoracic kyphosis |
Source: Roussouly & Pinheiro-Franco, European Spine Journal, 2011
Spinal profiles determine the physiological pelvic orientation and the natural balance profile specific to each subject. A seat that ignores this morphological reality inevitably generates compensations.
3. The natural balance profile
Every individual has their own sagittal organization, determined notably by their pelvic incidence, the spontaneous orientation of their pelvis, and the natural distribution of their spinal curves. This configuration is what the SBNFA™ doctrine defines as the natural balance profile.
In a standing position, this profile is maintained largely unconsciously by the locomotor system, because it corresponds to a functionally economical organization: constraints are distributed with minimal shear, neuromuscular expenditure is reduced, and the natural capacity for micro-adjustment is preserved.
A Type 1 subject naturally maintains their pelvis in slight retroversion while standing — this is their balance point. As soon as a seat prevents them from recovering this orientation, their body must actively compensate, at the cost of increased neuromuscular effort and concentrated mechanical constraints.
When a seat imposes an orientation incompatible with this natural balance profile, the body develops spinal, muscular, and fascial compensations designed to prevent postural collapse. This is not a flaw in the person — it is an adaptive response to a geometric constraint imposed from outside.
The SBNFA™ doctrine therefore does not seek to impose an ideal universal posture, but to restore the mechanical conditions that allow the subject to recover their own natural balance profile and their self-regulatory capacities.
Thus, despite their differences, all spinal profiles pursue the same goal: to keep the body’s center of gravity in a stable balance zone while minimizing energy expenditure.
This balance is not, however, determined solely by the curves of the spine.
It also depends on the orientation of the pelvis — the true interface between the spine and the lower limbs.
To understand what happens when we move from standing to seated, we must now focus on this central element of human balance: the pelvis.
4. The pelvis: the first vertebra of the spine
Having understood that each individual has their own pelvi-spinal organization, an essential question remains:
What happens to this organization when we move from standing to seated?
For a long time, the seated position was described as a simple hip flexion. The subject bends their lower limbs, settles onto a seat, and maintains their balance through the combined action of the trunk and lower limb muscles. This representation is, however, incomplete.
Research on sagittal balance shows that the pelvis actively participates in this transition. When we sit down, it does not remain stationary. Its orientation changes to allow the body to adapt to a new mechanical organization.
In other words, the seated position does not simply correspond to a change in posture: it constitutes a genuine reorganization of the pelvi-spinal system.
4.1. Moving to a seated position modifies pelvic orientation
Studies on the relationships between the spine, pelvis, and hips show that the transition from standing to seated is accompanied by an increase in pelvic version: the pelvis progressively tilts backward.
This rotation is not a minor phenomenon. It directly participates in the body’s adaptation to the new geometry imposed by hip flexion and the displacement of the base of support.
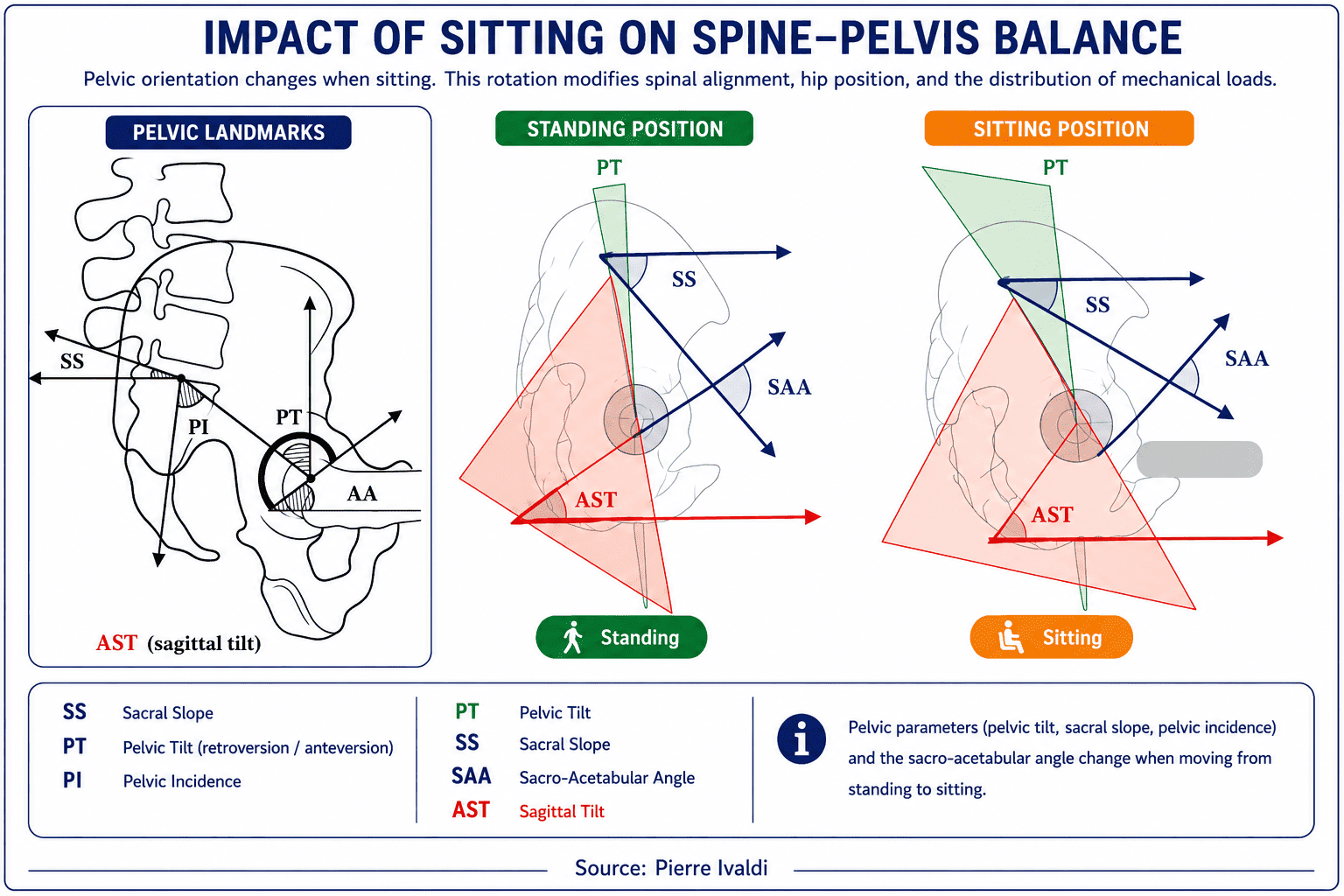
The observation of these parameters reveals a fundamental point: when an individual sits down, their pelvis changes orientation in order to allow the rest of the musculoskeletal system to maintain its balance.
The seated position therefore does not correspond to a simple arrest of movement.
On the contrary, it requires permanent adaptation of pelvic organization.
4.2. Pelvic version: an adaptation mechanism
Radiographic studies allow this transformation to be directly visualized.
In the subject shown in the figure below, pelvic version increases from approximately 10° in the standing position to more than 24° in the seated position.

This increase in pelvic version reflects a posterior rotation of the pelvis.
This movement simultaneously modifies:
- hip position;
- the organization of spinal curves;
- the distribution of mechanical loads;
- the muscular strategies used to maintain balance.
The pelvis thus appears as a true mechanical adaptation organ situated at the interface between the spine and the lower limbs.
4.3. Why this observation is fundamental
This evolution of pelvic version has a major consequence.
It shows that the pelvis cannot be studied independently of the hips.
When the pelvis changes orientation, the mechanical relationships between the pelvis and femurs change immediately.
Conversely, any modification of the position of the lower limbs in turn influences the way in which the pelvis can organize itself.
The pelvis and femurs therefore form an inseparable system.
This relationship is essential for understanding the seated position.
For if pelvic balance depends directly on its relationship with the lower limbs, then knee height, thigh inclination, and hip opening become determining parameters.
Before even discussing seated posture, pain, or ergonomic settings, it is necessary to understand this true biomechanical crossroads: the pelvis-femur couple.
5. The pelvis-femur couple: the true biomechanical crossroads
The pelvis never works alone. In a seated position, its orientation depends directly on its relationship with the femurs.
This relationship constitutes a central point of understanding. If the femurs impose an orientation incompatible with the pelvis’s natural profile, the spine will need to compensate. Conversely, when the pelvis-femur relationship remains coherent, the pelvis can more easily recover its functional balance zone.
This point allows us to move beyond an overly simplistic view of seated ergonomics. The question is not only whether the back is straight, whether the backrest is inclined, or whether the feet touch the floor.
The fundamental question becomes: in what relationship is the pelvis placed relative to the femurs?
It is this relationship that conditions pelvic orientation, hip mobility, the spine’s ability to maintain its functional curves, and the possibility of making small continuous adjustments.
The pelvis-femur couple must therefore be understood as a mechanical interface. It connects the spine to the lower limbs and determines the conditions under which the pelvis can remain mobile, stable, and adaptable.
6. Why recommendations speak of 90° to 110°
Ergonomic recommendations often refer to a trunk-thigh opening of between 90° and 110°, sometimes more depending on the situation.
These recommendations are not unreasonable. They generally aim to avoid excessive rounding of the lumbar spine, to limit prolonged trunk flexion, and to reduce certain disc constraints.
But they do not address exactly the same parameter as the SBNFA™ doctrine: whereas classical ergonomics observes the trunk-thigh angle or the apparent angle between the backrest and the seat, SBNFA™ focuses on the relationship between the pelvic plane and the femoral axis — a distinction whose biomechanical implications are developed in section 9.
The same trunk-thigh angle can correspond to very different pelvic organizations depending on whether the pelvis is retroverted, vertical, or anteverted.
This is why the 90° reference between the thighs and the pelvic plane should not be understood as a fixed L-shaped posture imposed by a standard chair.
It should be understood as a reference for anatomical relationship, to be adapted according to the subject’s sagittal profile.
The 90° in question here is not the 90° backrest-to-seat angle. It is a functional reference of the pelvis-femur couple, which must remain compatible with the natural pelvic orientation.
7. Why knees should not be at the same height for everyone
If the natural pelvic orientation varies from one subject to another, then the position of the femurs cannot be strictly identical for everyone.
This is where knee height becomes an essential parameter.
For a profile with a retroverted tendency, the pelvis naturally seeks a more posterior orientation. In this case, slightly higher knees can help respect this organization and limit the appearance of lumbar compensations.
For a more vertical profile, a knee height close to that of the hips may be more consistent with the pelvis’s natural organization.
For a profile with an anteverted tendency, lower knees may on the contrary prevent the pelvis’s natural forward orientation from being disrupted.
This logic does not aim to impose a universal rule.
It aims to adapt the seating geometry to the subject’s pelvi-spinal organization.
What is often called good seated posture should therefore be understood differently: not as a single position, but as a coherent relationship between the pelvis, femurs, and the body’s adaptive capacities.
8. Behavior of spinal profiles in standard seated posture
In standard seated posture — 90° between backrest and seat, knees at hip height — spinal profiles are progressively constrained into orientations incompatible with their natural balance profile. The body responds by developing compensations that, over time, become a source of chronic pain.
A. Profile-by-profile analysis
| Profile | Behavior in standard seated posture | Spinal compensation | Clinical consequences |
|---|---|---|---|
| Type 1 (natural retroversion) | Retroversion blocked — pelvis cannot tilt backward | Compensatory lumbar kyphosis | ↑ posterior disc pressure, possible pudendal neuralgia (Barrey et al., 2013) |
| Type 3 / 4 (natural anteversion) | Anteversion limited — pelvis cannot tilt forward | Compensatory lumbar hyperextension | ↑ facet joint pressure, cluneal neuralgia (Roussouly et al., 2011; Clays et al., 2017) |
| Type 2 (vertical pelvis) | Vertical pelvis but unstable without appropriate support | Increased compensatory muscle activity | Early fatigue of spinal erectors (Versteeg et al., 2016) |
B. The progressive compensation mechanism
These compensations do not appear suddenly. They develop progressively, over hours of daily sitting, according to a three-stage process that the SBNFA™ doctrine identifies as the postural degradation cycle:
- Phase 1 — Geometric constraint: the seat imposes an orientation incompatible with the natural balance profile. The body actively resists.
- Phase 2 — Neuromuscular compensation: the paraspinal muscles, hip flexors, and pelvi-spinal stabilizers mobilize to maintain an acceptable balance. Neuromuscular cost increases.
- Phase 3 — Structural adaptation: in the case of repeated and poorly variable constraints, the fascia and passive structures (discs, ligaments) undergo progressive modifications of their mechanical properties — loss of glide, densification of connective tissue, focal hyperpressure.
It is not only the intensity of the constraints that matters, but their repetition and low variability: a static seat generates identical mechanical loads hour after hour, with no possibility of redistribution.
In standard seated posture, spinal profiles are progressively distanced from their natural balance profile. Pain is not a sign of pathology — it reflects a mechanical mismatch between the subject’s morphology and the geometric constraints imposed by the seat.
This standardized corrective logic is now very widespread. Dr. Jason Lowenstein, in his article “How to Correct Anterior Pelvic Tilt (Lumbar Lordosis)”, presents pelvic anteversion as a postural abnormality associated with muscular imbalances — to be corrected through targeted exercises. This approach is extremely common in the Anglo-Saxon world, particularly in rehabilitation, fitness, and physical preparation settings.
Yet research on sagittal profiles shows that it falls short as soon as it treats certain natural morphologies as inherently pathological. In a Type 3 or 4 profile (high PI), anteversion and hyperlordosis are not a muscular imbalance: they are the structural mechanical solution imposed by the bony architecture, permanently fixed at puberty. Correcting this “anomaly” means eliminating a necessary compensation — at the cost of destabilizing the entire chain.
Ref.: Lowenstein, J. — “How to Correct Anterior Pelvic Tilt (Lumbar Lordosis)”; see also Roussouly & Pinheiro-Franco, European Spine Journal, 2011.
9. The biomechanical optimum of the pelvis-femur couple
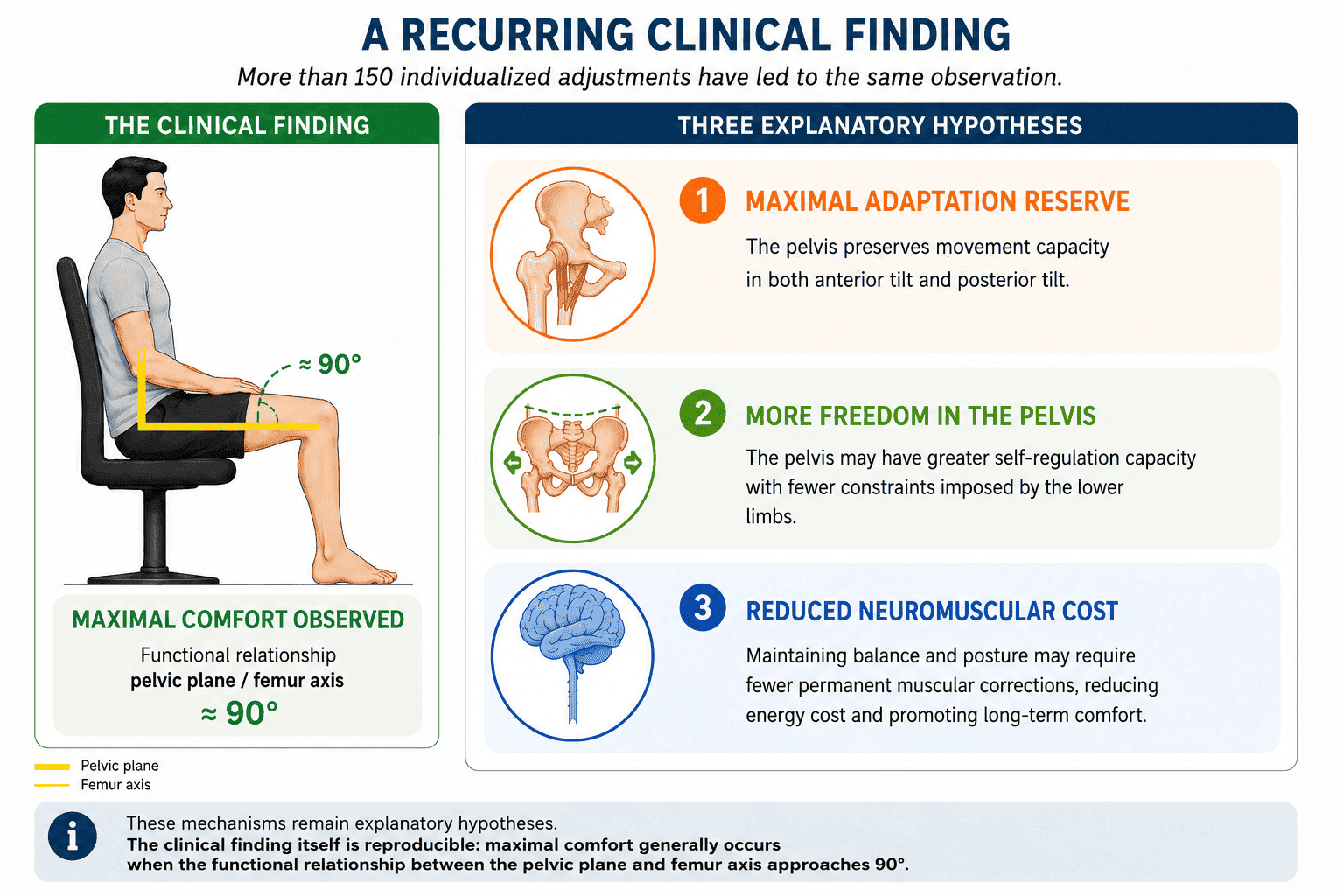
Beyond pelvic orientation in the sagittal plane, the SBNFA™ doctrine identifies a second fundamental biomechanical parameter: the femoro-pelvic angle — the angle formed between the femoral axis and the pelvic plane. Several independent bodies of work converge toward 90° as a biomechanical reference value.
Important clarification: the 90° reference mentioned here does not correspond to the angle between the backrest and the seat, nor simply to the trunk-thigh opening. It concerns the relationship between the pelvic plane and the femoral axis. Ergonomic recommendations often mention a trunk-thigh opening of 90° to 110°; the SBNFA™ doctrine, by contrast, is concerned with the functional coherence of the pelvis-femur couple according to the subject’s natural profile.
A. Definition and importance of the femoro-pelvic angle
The pelvic plane is defined by the iliac crests and the sacrum; the femoral axis, by the femoral head and condyles. The femoro-pelvic angle corresponds to the angle formed between these two biomechanical axes in the sagittal plane.
B. Why 90°?
Three bodies of work provide elements compatible with this reference value:
- Neuromuscular economy — the work of Versteeg et al. (2016) suggests that hip-trunk coordination optimizes muscular lever arms when the pelvis-femur relationship remains within a coherent functional zone — compatible with the 90° hypothesis.
- Intradiscal decompression — Clays et al. (2017) show that an adapted seat inclination reduces lumbar intradiscal pressures — which is consistent with the hypothesis that restoring the femoro-pelvic angle toward 90° produces a similar decompression effect.
- Preservation of the neutral zone — Panjabi’s (1992) neutral zone theory provides a compatible theoretical framework: when mechanical constraints remain within an optimal functional zone, the passive structures of the spine can fulfill their stabilizing role without overactivation — a logic that the 90° hypothesis seeks to extend to the seated position.
Beyond these data from the scientific literature, a recurring clinical observation has emerged during individualized adjustments carried out according to the SBNFA™ approach. Regardless of spinal profile or pelvic incidence, maximum comfort generally appears when the functional relationship between the pelvic plane and the femoral axis approaches 90°. Several mechanisms may contribute to explaining this observation. At this stage, these are explanatory hypotheses compatible with current data, but the clinical finding itself is remarkably reproducible.
In standard flat seating — knees horizontally aligned with the hips — this optimum can only be maintained for the Type 2 profile (naturally vertical pelvis). For Types 1 and 3/4, flat seating geometry mechanically generates a deviation from this optimum, which explains why these profiles systematically develop compensations during prolonged sitting.
The 90° angle between the femur and the pelvic plane appears as a biomechanical balance crossroads. It seems to correspond to a favorable functional zone, associated with better distribution of constraints, reduced neuromuscular cost, and the maintenance of an adaptive reserve for the pelvis and spine.
This theoretical convergence is consistent with a field observation: during individualized accompaniment in the handling and morphological adjustment of the seat, restoring this 90° angle produces an immediate and convergent sensation in subjects. The body “falls into place” — a spontaneous postural recognition sensation, without conscious effort, accompanied by the disappearance of habitual tensions. This proprioceptive signal, observed recurrently across more than one hundred and fifty different morphological profiles, is compatible with the model: when seating geometry ceases to work against the natural structure and instead liberates it, the nervous system signals this immediately.
10. Dynamic SBNFA™ solutions: restoring self-regulated balance
The SBNFA™ doctrine rests on two complementary biomechanical principles, operating simultaneously: restoring the pelvic orientation corresponding to the subject’s natural balance profile, and maintaining the femoro-pelvic angle at 90° through dynamic adjustment of the lower limbs.
10.1. Adaptive sagittal wedging: adjustment to Roussouly profiles
The use of removable wedges, positioned at the front or rear of the cushion according to sagittal typology, acts specifically on the inclination of the pelvis in the sagittal plane.
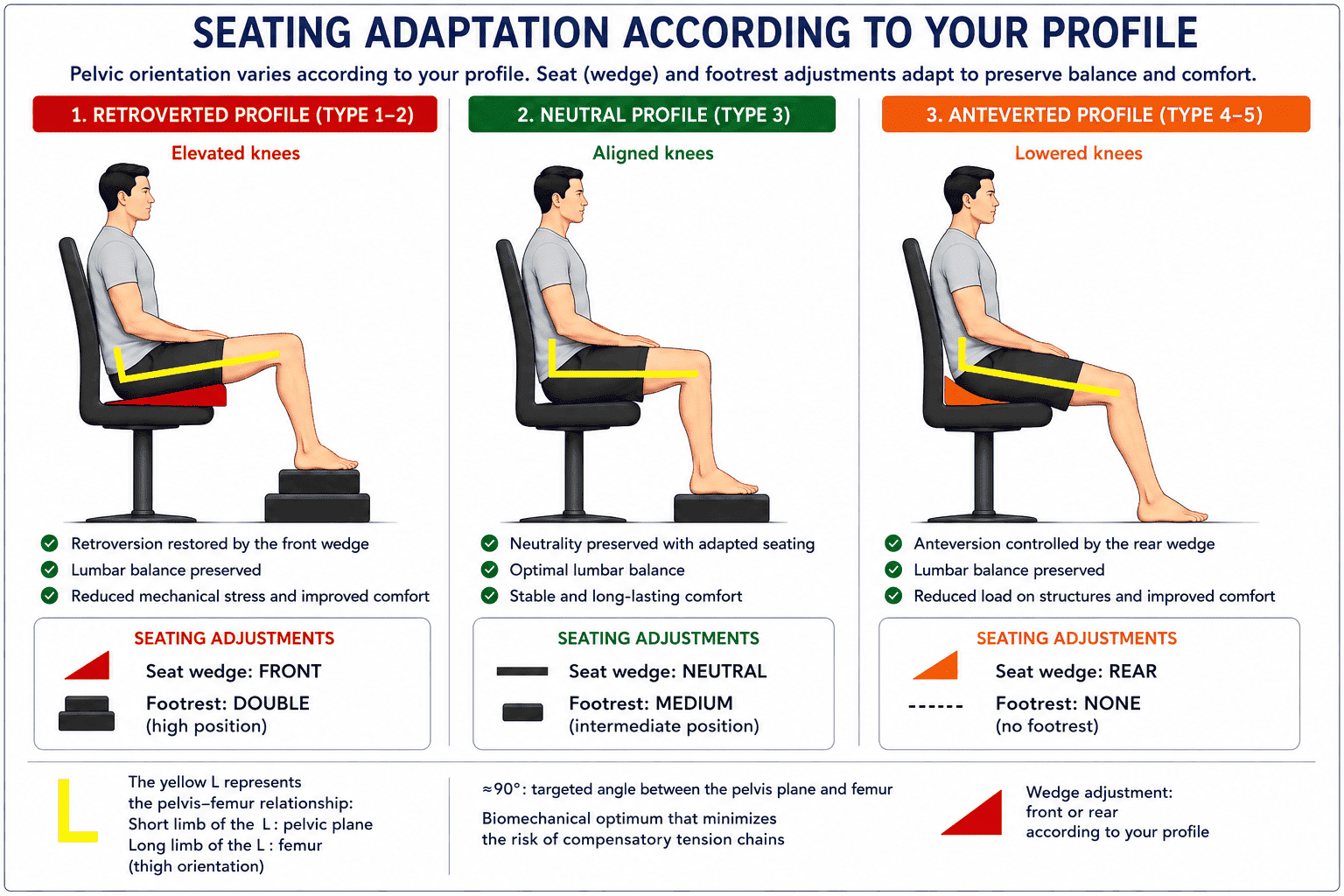
| Profile | SBNFA™ solution | Effect on femoro-pelvic angle | Result |
|---|---|---|---|
| Type 1 (retroversion) | Wedge under front of cushion + raised knees | Compensates posterior pelvic tilt → angle = 90° | Self-regulated balance, limitation of compensatory lumbar kyphosis |
| Type 3 / 4 (anteversion) | Wedge under rear of cushion + lowered knees | Compensates anterior pelvic tilt → angle = 90° | Self-regulated balance, limitation of lumbar hyperextension |
| Type 2 (vertical pelvis) | Knees at same height as hips | Angle naturally at 90° | Self-regulated balance, physiological lordosis preserved |
By restoring the pelvic orientation corresponding to the subject’s natural balance profile, this system limits detrimental spinal compensations and maintains the 90° biomechanical optimum of the femoro-pelvic angle. The SBNFA™ system does not aim to lock the pelvis in a fixed position, but to restore a stable mechanical environment allowing the nervous system to spontaneously recover its natural adaptation strategies.
10.2. The Exobase® with 4 independent pads: a new spino-pelvic dynamic
While the wedges stabilize the pelvis in the sagittal plane, the multi-articulated Exobase® with 4 independent pads frees the physiological micro-adjustments in the horizontal plane.
Unlike a monolithic seat that locks the support of the thighs and pelvis together, Aporia® dissociates the four main support zones of the pelvis-lower limb complex: left ischium, right ischium, left thigh, and right thigh.
Each pad is mounted on a multidirectional ball joint allowing it to orient freely through 360°. This architecture avoids the mechanical locking typically imposed by conventional seats and allows independent adaptations of the hips, pelvis, and spine.

Biomechanical consequences for spino-pelvic dynamics
The biomechanical consequences of this dissociation of support zones concern primarily three domains: hip freedom, pelvic mobility, and permanent adaptation of the spino-pelvic system.
1. Hip freedom
Coxo-femoral mobility — The independence of each pad finally allows, in a seated position, mobility of the coxo-femoral joint. As a result, the hips can participate in balance regulation, as they do in natural postures such as standing, squatting, cross-legged sitting, or kneeling.
Neutralization of torsion — By eliminating the torsional couple transmitted from the thigh to the pelvis by rigid seats, the system preserves pelvic symmetry and prevents rotational repercussions on the lumbar and thoracic segments.
Limitation of spinal compensations — This freedom allows the femur to find its physiological axis, limiting the mechanical compensations likely to propagate to the pelvis and then to the spine.
2. Pelvic mobility
Adaptability to sacral movement — The independence of the gluteal pads allows accommodation of the phenomena of nutation (anterior sacral tilt) and counter-nutation (posterior sacral tilt).
Fluidity of the pelvic cycle — By allowing autonomous mobility of the support zones, the system avoids locking of the sacroiliac joint and promotes the fluidity of the nutation and counter-nutation cycles involved in the absorption and transmission of spinal constraints.
Respect for spinal profiles — By accompanying mobility rather than imposing a fixed posture, the system promotes the maintenance of the natural adaptive capacities specific to each spinal profile.
3. Permanent adaptation
Management of asymmetries — The system allows each thigh pad to adapt to length asymmetries, whether structural or functional, without causing compensatory pelvic tilting.
Variability of support — The autonomous management of pressures for each segment — thighs and buttocks, left and right — limits shear constraints at cutaneous interfaces and soft tissues, ensuring dynamic management of lateral load transfers.
Neuro-fascial continuity — The freedom of movement of the pads respects the continuity of mechanical adaptations of the hip-pelvis-spine complex and limits tissue blockages likely to impede natural spinal adjustments.
This architecture transforms the seat into a dynamic system capable of adapting to pelvic kinematics, rather than forcing the spine to adjust to a fixed geometry.
10.3. Dynamic adjustment of the lower limbs
Durable restoration of the natural balance profile can only be achieved if the coxo-femoral joint functions under optimal biomechanical conditions. Adjusting knee height constitutes the second operational pillar of the SBNFA™ doctrine.
In standard flat seating, the femoro-pelvic optimum of 90° can only be maintained for the Type 2 profile. The SBNFA™ approach resolves this impasse through a coordinated adjustment of knee height according to profile:
- Anteverted profiles (Types 3/4): restoring physiological anteversion tilts the pelvis forward. The knees must therefore be slightly lowered to preserve the femoro-pelvic angle at 90° and avoid compensations in lumbar hyperextension.
- Retroverted profiles (Type 1): restoring physiological retroversion tilts the pelvis backward. The knees must therefore be slightly raised to maintain femoro-pelvic balance and limit the appearance of compensatory lumbar kyphosis.
Adjusting knee height is therefore not a simple comfort detail, but an essential biomechanical condition for stabilizing the natural balance profile. This three-dimensional geometry allows shear constraints to be limited while enabling the deployment of self-regulated balance at reduced neuromuscular cost.
Unlike static devices or uncontrolled unstable systems, the SBNFA™ bioactive interface requires a progressive period of adaptation. This phase corresponds to a reorganization of neuromuscular, proprioceptive, and myofascial strategies induced by the new distribution of mechanical constraints.
In some chronically painful or hyperreactive subjects, this adaptation may require several weeks before achieving a stable functional balance. This period is not a sign of the device’s inadequacy — it reflects the neuromuscular and fascial plasticity of the locomotor system in the face of a renewed mechanical environment.
11. Conclusion: the inverted paradigm
The SBNFA™ doctrine reintroduces the seated position into a logic of living movement rather than rigid stabilization. Its approach rests on four complementary biomechanical steps:
- Identify the subject’s native sagittal profile according to the Roussouly classification.
- Analyze the compensations induced by standardized seating.
- Restore the natural balance profile through adaptive wedging and freedom of three-dimensional micro-adjustment.
- Optimize the femoro-pelvic angle to 90° through dynamic adjustment of the lower limbs.
The foundations of this approach draw on major works devoted to sagittal balance (Roussouly, 2011), neuromuscular spinal stabilization (Panjabi, 1992; Versteeg, 2016), and the biomechanical constraints of the seated position (Clays, 2017; Nachemson, 1981).
The paradigm is inverted: the body is no longer asked to adapt to an imposed static constraint — the interface adapts systemically to the subject’s neuro-postural typology. The fundamental objective of the SBNFA™ doctrine is not to impose an ideal universal posture, but to restore the mechanical conditions allowing the locomotor system to recover its natural self-regulatory capacities.
Understanding this changes the question we ask. No longer: “how do we correct this person?” But: “does this seat respect who they are?” This shift appears simple — it is in reality fundamental. And it is precisely this shift that the SBNFA™ doctrine proposes to make operational.
Identify your spinal profile
The real question then becomes simple: does your seat respect your natural balance profile… or gradually work against it?
👉 Analyze the mechanisms involved in your seated pain through our expert system — then discover which Aporia® solution may be best suited to your spinal profile.
Frequently asked questions
What is Roussouly’s spinal profile?
Why can the same seat suit some people and not others?
What is the femoro-pelvic angle and why is 90° optimal?
How does the SBNFA™ doctrine differ from classical ergonomic approaches?
Can pudendal or cluneal neuralgia be linked to seated posture?
How long does the adaptation period to a bioactive seat last?
Further reading
Explore on Blue Portance
- ➡️ Understanding fascia and tensegrity: « The invisible system of constraint and pain regulation »
- ➡️ The importance of micro-movements: « Why moving a little is more important than moving a lot »
- ➡️ Chronic Pain Part 1: « Chronic pain decoded: understanding the mechanisms to finally act »
Scientific references
- Barrey, C., et al. (2013). Sagittal balance of the pelvis-spine complex and its importance in spinal surgery. Journal of Orthopaedic Science, 18(2), 140–147. [DOI]
- Clays, E., et al. (2017). The effect of seat pan tilt on spinal loads and comfort in sitting. Journal of Biomechanics, 58, 123–129. [DOI]
- Labat, J. J., et al. (2008). Anatomical study of the pudendal nerve and its surgical implications in pudendal neuralgia. Neurosurgery, 62(4), 985–991. [DOI]
- Lengsfeld, M., et al. (2000). Spinal load changes during rotatory dynamic sitting. Clinical Biomechanics, 15(5), 321–328. [DOI]
- Nachemson, A. (1981). Disc pressure measurements. Spine, 6(1), 93–97. [DOI]
- Panjabi, M. M. (1992). The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. Journal of Spinal Disorders, 5(4), 383–389. [DOI]
- Roussouly, P., & Pinheiro-Franco, J. L. (2011). Sagittal parameters of the spine: Biomechanical approach. European Spine Journal, 20(Suppl 5), 598–608. [DOI]
- Versteeg, A. C., et al. (2016). Hip and trunk coordination in balance regulation during standing and sitting. Gait & Posture, 45, 11–16. [DOI]
© Blue Portance. Reproduction and distribution authorized for non-commercial purposes, provided the source is cited: “Blue Portance – SBNFA™ Doctrine”.